1] Studies Coordinating Centre, Division of Hypertension and Cardiovascular Rehabilitation, KU Leuven Department of Cardiovascular Sciences, University of Leuven, Leuven, Belgium [2] Hypertension Unit, Department of Internal Medicine, University of Kinshasa Hospital, Kinshasa, Democratic Republic of Congo.
J Hum Hypertens. 2013 Dec;27(12):729-35. doi: 10.1038/jhh.2013.56. Epub 2013 Jun 27.
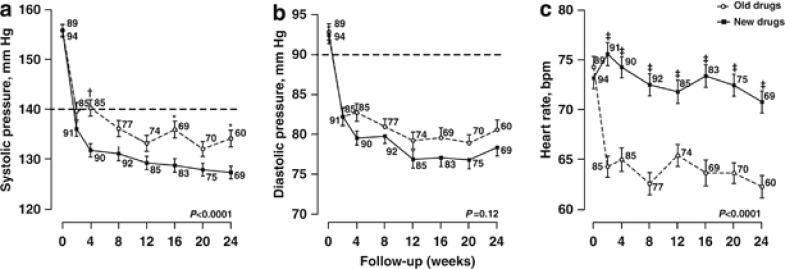
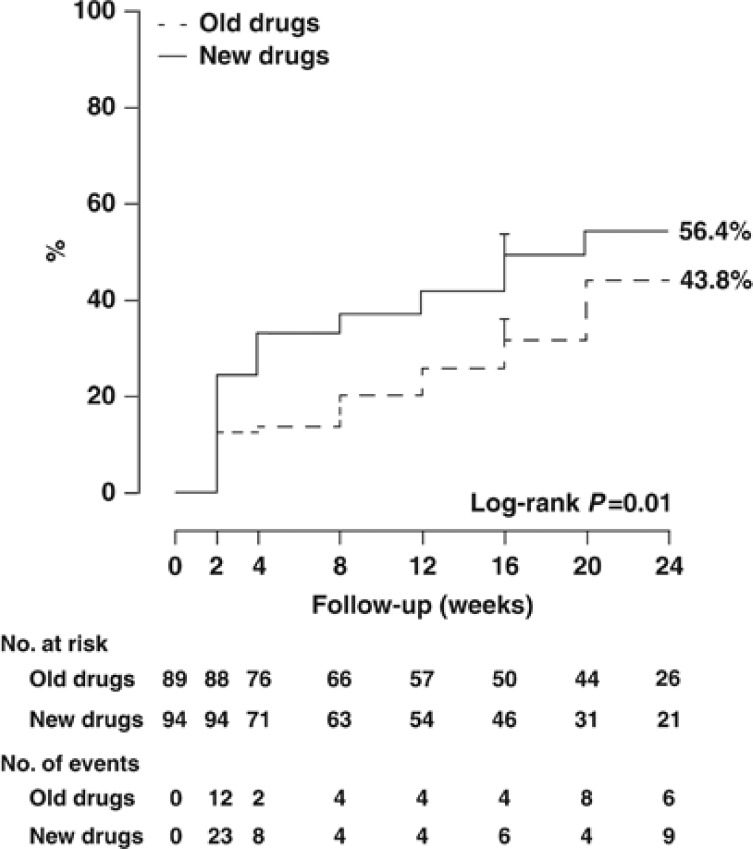
To address the epidemic of hypertension in blacks born and living in sub-Saharan Africa, we compared in a randomised clinical trial (NCT01030458) single-pill combinations of old and new antihypertensive drugs in patients (30-69 years) with uncomplicated hypertension (140-179/90-109 mm Hg). After ≥4 weeks off treatment, 183 of 294 screened patients were assigned to once daily bisoprolol/hydrochlorothiazide 5/6.25 mg (n=89; R) or amlodipine/valsartan 5/160 mg (n=94; E) and followed up for 6 months. To control blood pressure (<140/<90 mm Hg), bisoprolol and amlodipine could be doubled (10 mg per day) and α-methyldopa (0.5-2 g per day) added. Sitting blood pressure fell by 19.5/12.0 mm Hg in R patients and by 24.8/13.2 mm Hg in E patients and heart rate decreased by 9.7 beats per minute in R patients with no change in E patients (-0.2 beats per minute). The between-group differences (R minus E) were 5.2 mm Hg (P<0.0001) systolic, 1.3 mm Hg (P=0.12) diastolic, and 9.6 beats per minute (P<0.0001). In 57 R and 67 E patients with data available at all visits, these estimates were 5.5 mm Hg (P<0.0001) systolic, 1.8 mm Hg (P=0.07) diastolic and 9.8 beats per minute (P<0.0001). In R compared with E patients, 45 vs 37% (P=0.13) proceeded to the higher dose of randomised treatment and 33 vs 9% (P<0.0001) had α-methyldopa added. There were no between-group differences in symptoms except for ankle oedema in E patients (P=0.012). In conclusion, new compared with old drugs lowered systolic blood pressure more and therefore controlled hypertension better in native African black patients.
为解决撒哈拉以南非洲出生和生活的黑人高血压流行问题,我们在一项随机临床试验(NCT01030458)中比较了新老降压药单药联合治疗无并发症高血压(140-179/90-109mmHg)患者的疗效。在停药≥4 周后,对 294 名筛查患者中的 183 名患者进行了一次每日服用比索洛尔/氢氯噻嗪 5/6.25mg(n=89;R)或氨氯地平/缬沙坦 5/160mg(n=94;E)的分组,并随访 6 个月。为了控制血压(<140/<90mmHg),比索洛尔和氨氯地平可以加倍(每天 10mg),并加用α-甲基多巴(每天 0.5-2g)。R 组患者的收缩压下降 19.5/12.0mmHg,E 组患者下降 24.8/13.2mmHg,R 组患者心率下降 9.7 次/分,E 组患者无变化(-0.2 次/分)。组间差异(R 组减去 E 组)为 5.2mmHg(P<0.0001)收缩压,1.3mmHg(P=0.12)舒张压和 9.6 次/分(P<0.0001)。在 57 名 R 组和 67 名 E 组中有全部访视点数据的患者中,这些估计值分别为 5.5mmHg(P<0.0001)收缩压、1.8mmHg(P=0.07)舒张压和 9.8 次/分(P<0.0001)。与 E 组相比,R 组有 45%(P=0.13)进展到更高剂量的随机治疗,33%(P<0.0001)加用α-甲基多巴。除 E 组患者的踝部水肿(P=0.012)外,两组间无其他症状差异。总之,与旧药相比,新的降压药降低收缩压的幅度更大,因此能更好地控制非洲黑人原发性高血压患者的血压。