Center for Outcomes Research and Analytics, Henry Ford Health System, Detroit, Michigan, USA.
BMJ Open. 2013 Jun 26;3(6):e002843. doi: 10.1136/bmjopen-2013-002843.
While multiple studies have demonstrated variations in the quality of cancer care in the USA, payers are increasingly assessing structure-level and process-level measures to promote quality improvement. Hospital-acquired adverse events are one such measure and we examine their national trends after major cancer surgery.
Retrospective, cross-sectional analysis of a weighted-national estimate from the Nationwide Inpatient Sample (NIS) undergoing major oncological procedures (colectomy, cystectomy, oesophagectomy, gastrectomy, hysterectomy, lung resection, pancreatectomy and prostatectomy). The Agency for Healthcare Research and Quality Patient Safety Indicators (PSIs) were utilised to identify trends in hospital-acquired adverse events.
Secondary and tertiary care, US hospitals in NIS PARTICIPANTS: A weighted-national estimate of 2 508 917 patients (>18 years, 1999-2009) from NIS.
Hospital-acquired adverse events.
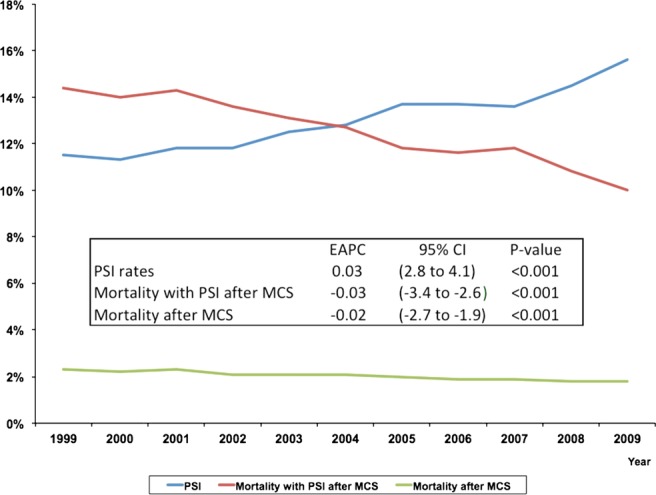
324 852 patients experienced ≥1-PSI event (12.9%). Patients with ≥1-PSI experienced higher rates of in-hospital mortality (OR 19.38, 95% CI 18.44 to 20.37), prolonged length of stay (OR 4.43, 95% CI 4.31 to 4.54) and excessive hospital-charges (OR 5.21, 95% CI 5.10 to 5.32). Patients treated at lower volume hospitals experienced both higher PSI events and failure-to-rescue rates. While a steady increase in the frequency of PSI events after major cancer surgery has occurred over the last 10 years (estimated annual % change (EAPC): 3.5%, p<0.001), a concomitant decrease in failure-to-rescue rates (EAPC -3.01%) and overall mortality (EAPC -2.30%) was noted (all p<0.001).
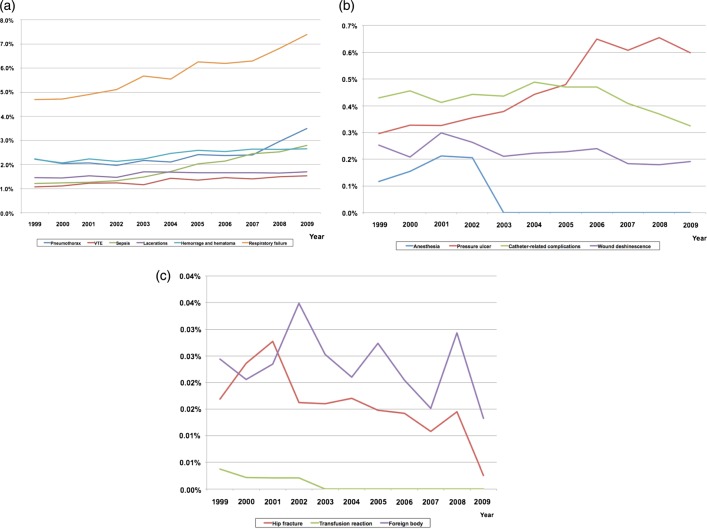
Over the past decade, there has been a substantial increase in the national frequency of potentially avoidable adverse events after major cancer surgery, with a detrimental effect on numerous outcome-level measures. However, there was a concomitant reduction in failure-to-rescue rates and overall mortality rates. Policy changes to improve the increasing burden of specific adverse events, such as postoperative sepsis, pressure ulcers and respiratory failure, are required.
尽管多项研究表明美国的癌症治疗质量存在差异,但支付方越来越多地评估结构层面和过程层面的措施以促进质量改进。医院获得性不良事件就是这样一种措施,我们在主要癌症手术后对其全国趋势进行了研究。
利用全国住院患者样本(NIS)的加权全国估计值进行回顾性、横断面分析,这些患者接受了主要肿瘤学手术(结肠切除术、膀胱切除术、食管切除术、胃切除术、子宫切除术、肺切除术、胰腺切除术和前列腺切除术)。利用医疗保健研究与质量患者安全指标(PSIs)来确定医院获得性不良事件的趋势。
美国 NIS 的二级和三级保健、医院。
来自 NIS 的 2508917 名(年龄>18 岁,1999-2009 年)加权全国估计值患者。
医院获得性不良事件。
324852 名患者经历了≥1-PSI 事件(12.9%)。发生≥1-PSI 的患者院内死亡率更高(OR 19.38,95%CI 18.44 至 20.37),住院时间延长(OR 4.43,95%CI 4.31 至 4.54)和过度医疗费用(OR 5.21,95%CI 5.10 至 5.32)。在低容量医院接受治疗的患者,PSI 事件和抢救失败率都更高。在过去 10 年中,主要癌症手术后 PSI 事件的频率稳步上升(估计每年百分比变化(EAPC):3.5%,p<0.001),但抢救失败率(EAPC-3.01%)和总死亡率(EAPC-2.30%)呈下降趋势(均 p<0.001)。
在过去的十年中,主要癌症手术后全国范围内潜在可避免的不良事件频率大幅增加,对众多结果层面的指标产生了不利影响。然而,抢救失败率和总死亡率也随之下降。需要采取政策措施来改善术后脓毒症、压疮和呼吸衰竭等特定不良事件的不断增加的负担。