Division of Clinical Microbiology, Mayo Clinic, 200 First Street SW, Rochester, MN, USA.
Malar J. 2013 Jul 8;12:231. doi: 10.1186/1475-2875-12-231.
The gold standard for malaria diagnosis is the examination of thick and thin blood films. Thick films contain 10 to 20 times more blood than thin films, correspondingly providing increased sensitivity for malaria screening. A potential complication of thick film preparations is sloughing of the blood droplet from the slide during staining or rinsing, resulting in the loss of sample. In this work, two methods for improving thick film slide adherence ('scratch' (SCM) and 'acetone dip' (ADM) methods) were compared to the 'standard method' (SM) of thick film preparation.
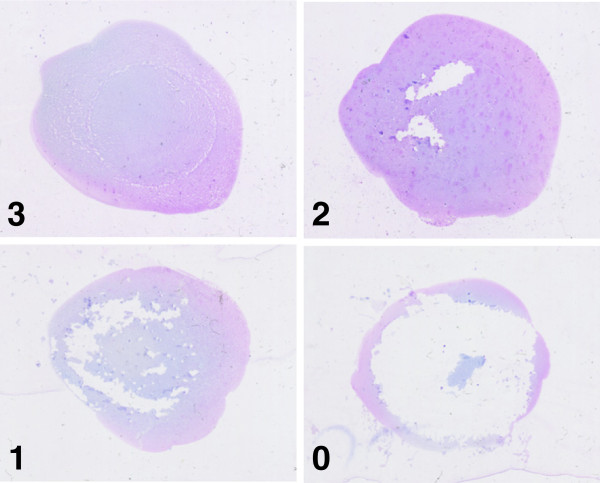
Standardized blood droplets from 26 previously examined EDTA whole blood specimens (22 positive and four negative) were concurrently spread on glass slides using the SM, ADM, and SCM. For the SM and ADM prepared slides, the droplet was gently spread to an approximate 22 millimeters in diameter spot on the slide using the edge of a second glass slide. For the SCM, the droplet was spread by carefully grinding (or scratching) it into the slide with the point of a second glass slide. Slides were dried for one hour in a laminar flow hood. For the ADM, slides were dipped once in an acetone filled Coplin jar and allowed to air dry. All slides were then Giemsa-stained and examined in a blinded manner. Adherence was assessed by blinded reviewers.
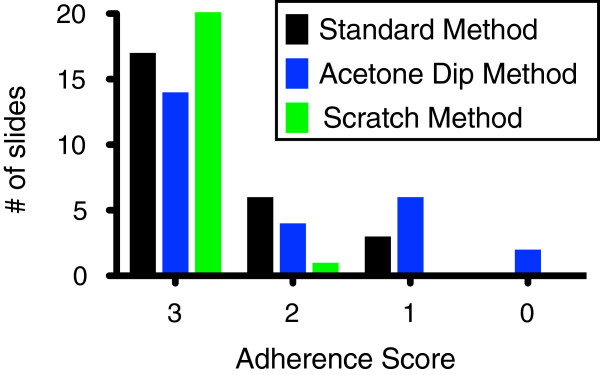
No significant or severe defects were observed for slides prepared with the SCM. In contrast, 8 slides prepared by the ADM and 3 prepared using the SM displayed significant or severe defects. Thick films prepared by the three methods were microscopically indistinguishable and concordant results (positive or negative) were obtained for the three methods. Estimated parasitaemia of the blood samples ranged from 25 to 429,169 parasites/μL of blood.
The SCM is an inexpensive, rapid, and simple method that improves the adherence of thick blood films to standard glass slides without altering general slide preparation, microscopic appearance or interpretability. Using the SCM, thick films can be reliably examined less than two hours after sample receipt. This represents a significant diagnostic improvement over protocols requiring extended drying periods.
疟疾诊断的金标准是检查厚血膜和薄血膜。厚血膜中的血液比薄血膜多 10 到 20 倍,相应地提高了疟疾筛查的灵敏度。厚血膜制备的一个潜在并发症是在染色或冲洗过程中血滴从载玻片上脱落,导致样本丢失。在这项工作中,比较了两种提高厚血膜载玻片附着力的方法(“划痕”(SCM)和“丙酮浸泡”(ADM)方法)与厚血膜制备的“标准方法”(SM)。
使用 SM、ADM 和 SCM 同时将来自 26 个先前检查过的 EDTA 全血标本(22 个阳性和 4 个阴性)的标准化血滴铺展在玻璃载玻片上。对于 SM 和 ADM 制备的载玻片,使用第二块玻璃载玻片的边缘轻轻将血滴铺展到载玻片上约 22 毫米的直径斑点上。对于 SCM,通过用第二块玻璃载玻片的尖端小心地将血滴磨(或刮)到载玻片上。将载玻片在层流罩中干燥一小时。对于 ADM,将载玻片浸入装满丙酮的 Coplin 罐中一次,然后让其风干。所有载玻片均用吉姆萨染色并以盲法进行检查。盲法评估人员评估了附着力。
未观察到 SCM 制备的载玻片出现明显或严重缺陷。相比之下,8 个 ADM 制备的载玻片和 3 个 SM 制备的载玻片显示出明显或严重的缺陷。用三种方法制备的厚血膜在显微镜下无法区分,并且三种方法均获得了一致的结果(阳性或阴性)。血液样本的估计寄生虫血症范围为 25 至 429,169 个寄生虫/μL 血液。
SCM 是一种廉价、快速且简单的方法,可提高厚血膜对标准玻璃载玻片的附着力,而不会改变一般载玻片的制备、显微镜下的外观或可解释性。使用 SCM,可以在样本接收后不到两小时可靠地检查厚血膜。这代表着在需要延长干燥期的方案方面的重大诊断改进。