Department of Medicine, University of Massachusetts Medical School, Worcester, MA 01605, USA.
Am J Med. 2013 Sep;126(9):798-804. doi: 10.1016/j.amjmed.2013.02.026. Epub 2013 Jul 5.
There are limited data informing the optimal treatment strategy for acute myocardial infarction in the oldest old (aged ≥85 years). The study aim was to examine whether decade-long increases in guideline-based cardiac medication use mediate declines in post-discharge mortality among oldest old patients hospitalized with acute myocardial infarction.
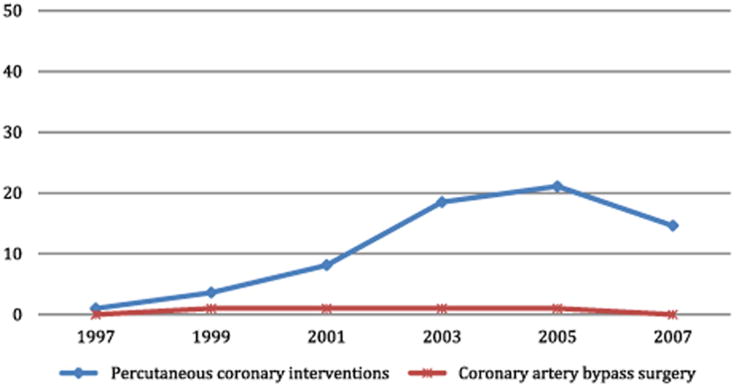
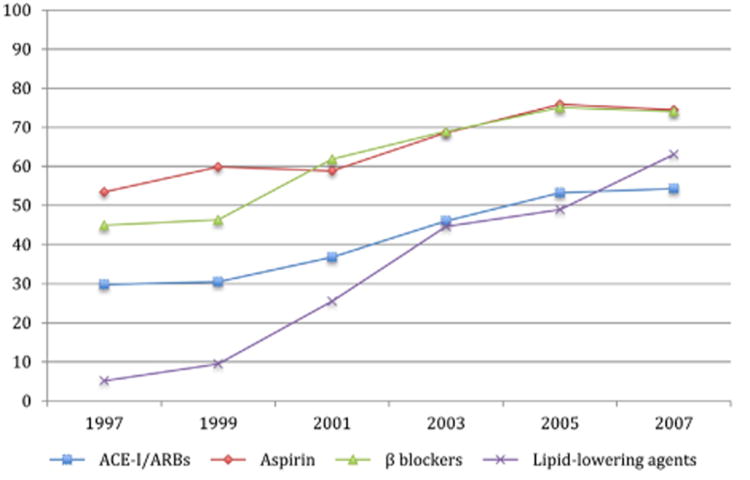
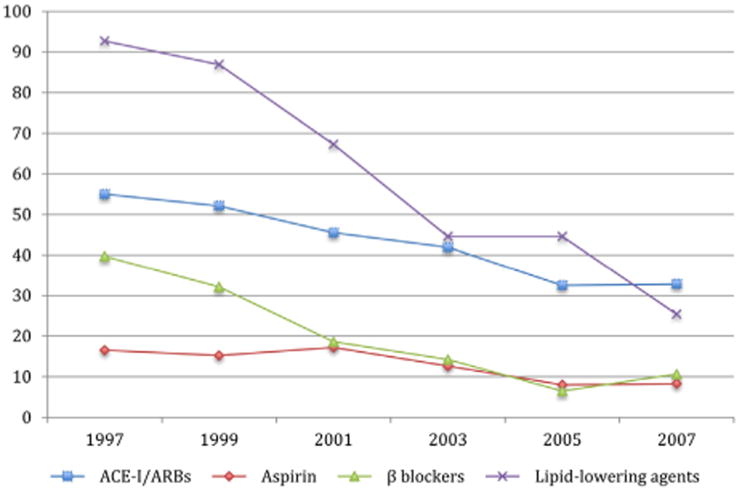
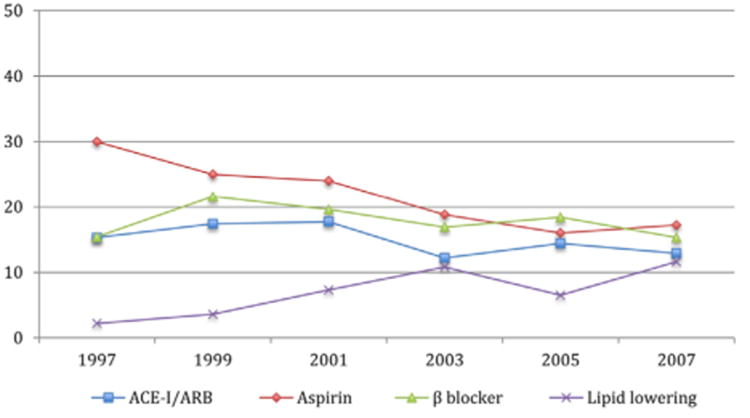
The study sample included 1137 patients aged ≥85 years hospitalized in 6 biennial periods between 1997 and 2007 for acute myocardial infarction at all 11 greater Worcester, Massachusetts, medical centers. We examined trends in 90-day survival after hospital discharge and guideline-based medication use (aspirin, angiotensin-converting enzyme inhibitors/angiotensin receptor blockers, beta-blockers, lipid-lowering agents) for acute myocardial infarction during hospitalization and at discharge. Sequential multivariable Cox regression models examined the relationship among guideline-based medication use, study year, and 90-day post-discharge survival rates.
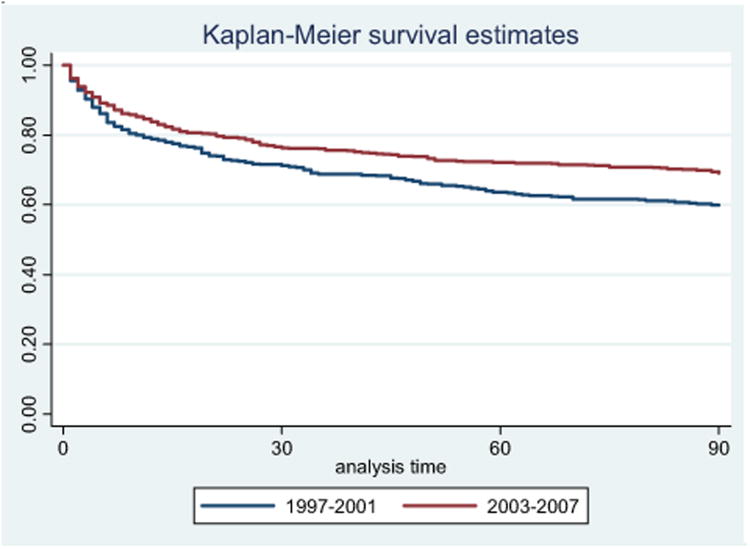
Patients hospitalized between 2003 and 2007 experienced higher 90-day survival rates than those hospitalized between 1997 and 2001 (69.1% vs 59.8%, P < .05). Between 1997 and 2007, the average number of guideline-based medications prescribed at discharge increased significantly (1.8 to 2.9, P < .001). The unadjusted hazard ratio for 90-day post-discharge mortality in 2003-2007 compared with 1997-2001 was 0.73 (95% confidence interval, 0.60-0.89); after adjustment for patient characteristics and guideline-based cardiac medication use, this relationship was no longer significant (hazard ratio, 1.26; 95% confidence interval, 1.00-1.58).
Between 1997 and 2007, 90-day survival improved among a population-based sample of patients aged ≥85 years hospitalized for acute myocardial infarction. This encouraging trend was explained by increased use of guideline-based medications.
对于年龄最大的老年人(≥85 岁),急性心肌梗死的最佳治疗策略的数据有限。本研究旨在探讨过去十年中基于指南的心脏药物治疗是否能降低因急性心肌梗死住院的最年长患者出院后的死亡率。
研究样本包括 1997 年至 2007 年期间在马萨诸塞州伍斯特市的 11 个医疗中心住院的 1137 名年龄≥85 岁的急性心肌梗死患者。我们检查了出院后 90 天生存率的趋势以及住院期间和出院时基于指南的药物使用(阿司匹林、血管紧张素转换酶抑制剂/血管紧张素受体阻滞剂、β受体阻滞剂、降脂药)。序贯多变量 Cox 回归模型探讨了基于指南的药物使用、研究年份和 90 天出院后生存率之间的关系。
2003 年至 2007 年期间住院的患者的 90 天生存率高于 1997 年至 2001 年期间住院的患者(69.1%比 59.8%,P<.05)。1997 年至 2007 年期间,出院时开具的基于指南的药物数量显著增加(1.8 至 2.9,P<.001)。2003-2007 年与 1997-2001 年相比,90 天出院后死亡率的未调整危险比为 0.73(95%置信区间,0.60-0.89);调整患者特征和基于指南的心脏药物使用后,这种关系不再显著(危险比,1.26;95%置信区间,1.00-1.58)。
在过去的十年中,因急性心肌梗死住院的年龄最大的老年患者(≥85 岁)的 90 天生存率有所提高。这一令人鼓舞的趋势归因于基于指南的药物治疗使用率的增加。