Schlimp Christoph J, Voelckel Wolfgang, Inaba Kenji, Maegele Marc, Ponschab Martin, Schöchl Herbert
Crit Care. 2013 Jul 12;17(4):R137. doi: 10.1186/cc12816.
Fibrinogen plays a key role in hemostasis and is the first coagulation factor to reach critical levels in massively bleeding trauma patients. Consequently, rapid estimation of plasma fibrinogen (FIB) is essential upon emergency room (ER) admission, but is not part of routine coagulation monitoring in many centers. We investigated the predictive ability of the laboratory parameters hemoglobin (Hb) and base excess (BE) upon admission, as well as the Injury Severity Score (ISS), to estimate FIB in major trauma patients.
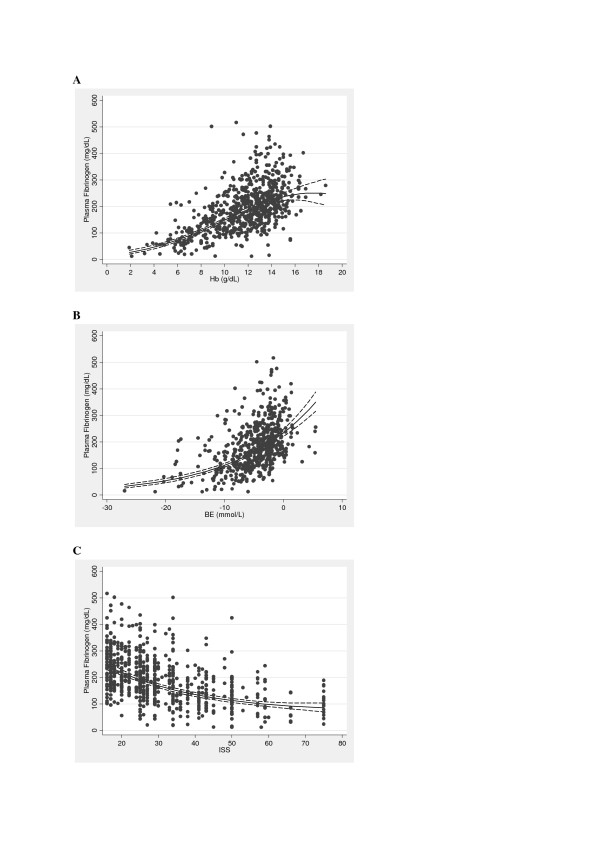
In this retrospective study, major trauma patients (ISS ≥16) with documented FIB analysis upon ER admission were eligible for inclusion. FIB was correlated with Hb, BE and ISS, alone and in combination, using regression analysis.
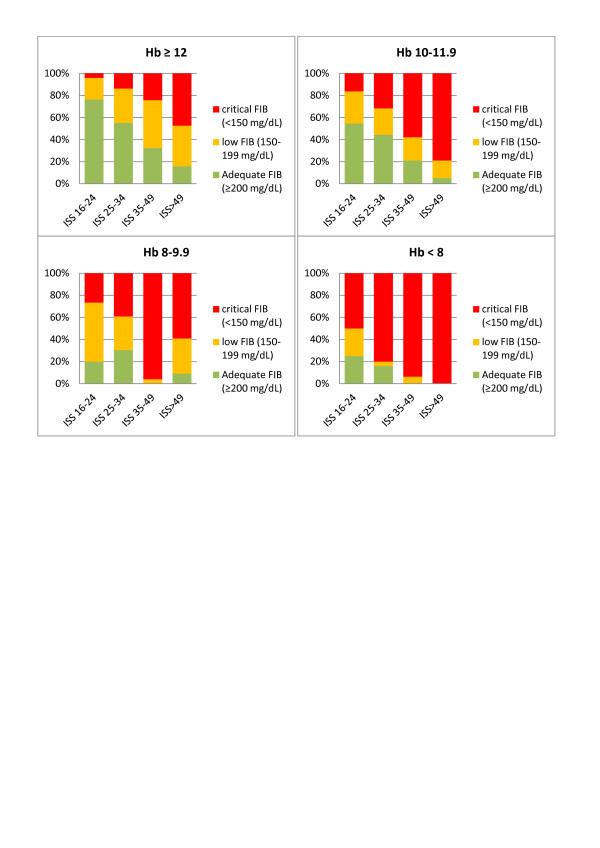
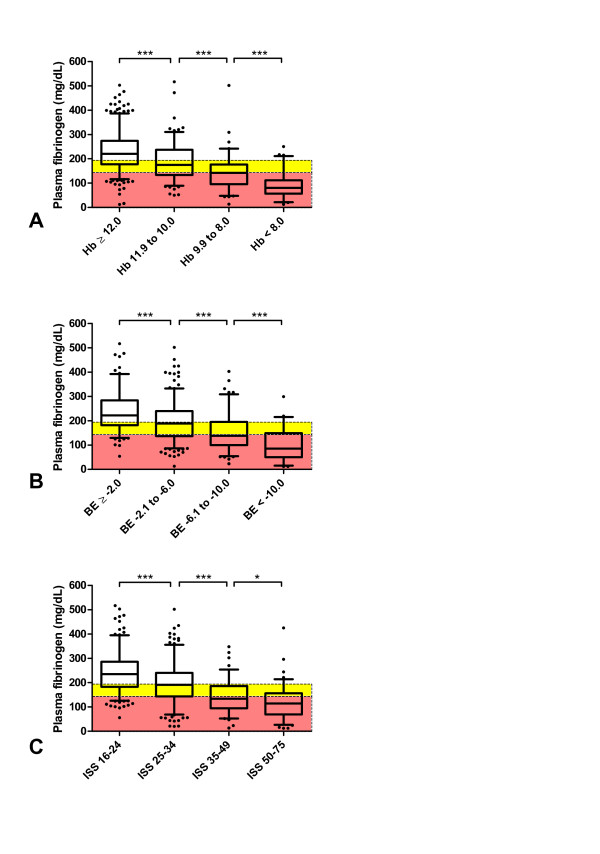
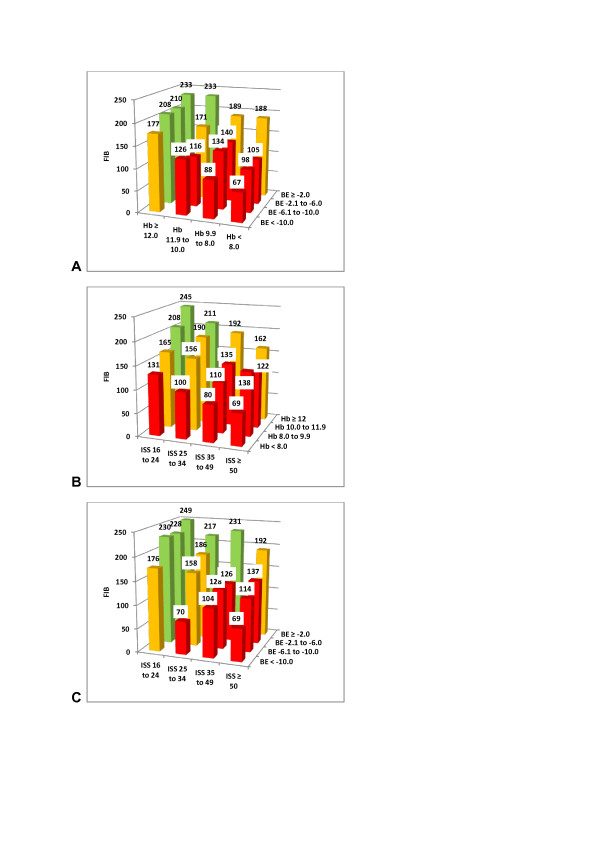
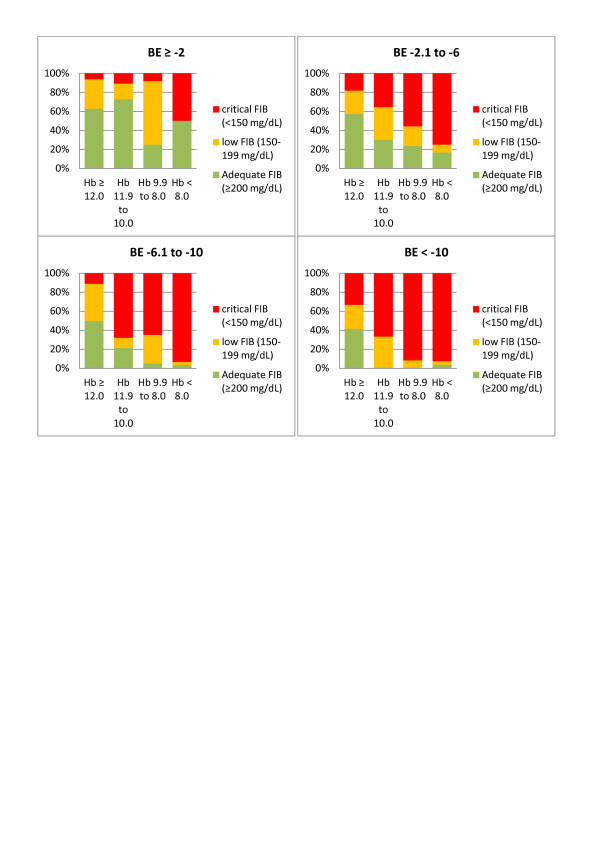
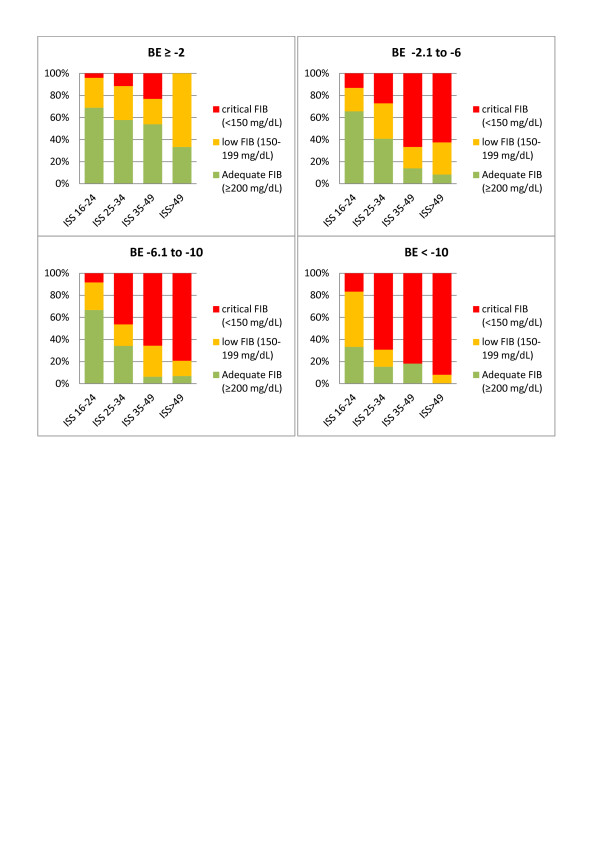
A total of 675 patients were enrolled (median ISS 27). FIB upon admission correlated strongly with Hb, BE and ISS. Multiple regression analysis showed that Hb and BE together predicted FIB (adjusted R2 = 0.46; loge(FIB) = 3.567 + 0.223.Hb - 0.007.Hb2 + 0.044.BE), and predictive strength increased when ISS was included (adjusted R2 = 0.51; loge(FIB) = 4.188 + 0.243.Hb - 0.008.Hb2 + 0.036.BE - 0.031.ISS + 0.0003.ISS2). Of all major trauma patients admitted with Hb <12 g/dL, 74% had low (<200 mg/dL) FIB and 54% had critical (<150 mg/dL) FIB. Of patients admitted with Hb <10 g/dL, 89% had low FIB and 73% had critical FIB. These values increased to 93% and 89%, respectively, among patients with an admission Hb <8 g/dL. Sixty-six percent of patients with only a weakly negative BE (<-2 mmol/L) showed low FIB. Of patients with BE <-6 mmol/L upon admission, 81% had low FIB and 63% had critical FIB. The corresponding values for BE <-10 mmol/L were 89% and 78%, respectively.
Upon ER admission, FIB of major trauma patients shows strong correlation with rapidly obtainable, routine laboratory parameters such as Hb and BE. These two parameters might provide an insightful and rapid tool to identify major trauma patients at risk of acquired hypofibrinogenemia. Early calculation of ISS could further increase the ability to predict FIB in these patients. We propose that FIB can be estimated during the initial phase of trauma care based on bedside tests.
纤维蛋白原在止血过程中起关键作用,是大量出血创伤患者中第一个达到临界水平的凝血因子。因此,在急诊室(ER)入院时快速估算血浆纤维蛋白原(FIB)至关重要,但在许多中心这并非常规凝血监测的一部分。我们研究了入院时实验室参数血红蛋白(Hb)和碱剩余(BE)以及损伤严重度评分(ISS)对主要创伤患者FIB的预测能力。
在这项回顾性研究中,符合条件纳入的是在ER入院时有记录FIB分析的主要创伤患者(ISS≥16)。使用回归分析将FIB与Hb、BE和ISS单独及联合进行相关性分析。
共纳入675例患者(ISS中位数为27)。入院时FIB与Hb、BE和ISS密切相关。多元回归分析表明,Hb和BE共同预测FIB(调整后R2 = 0.46;ln(FIB) = 3.567 + 0.223.Hb - 0.007.Hb2 + 0.044.BE),当纳入ISS时预测强度增加(调整后R2 = 0.51;ln(FIB) = 4.188 + 0.243.Hb - 0.008.Hb2 + 0.036.BE - 0.031.ISS + 0.0003.ISS2)。在所有入院时Hb <12 g/dL的主要创伤患者中,74%的患者FIB较低(<200 mg/dL),54%的患者FIB危急(<150 mg/dL)。入院时Hb <10 g/dL的患者中,89%的患者FIB较低,73%的患者FIB危急。在入院Hb <8 g/dL的患者中,这些值分别增至93%和89%。仅有轻度负BE(<-2 mmol/L)的患者中有66%显示FIB较低。入院时BE <-6 mmol/L的患者中,81%的患者FIB较低,63%的患者FIB危急。BE <-10 mmol/L时的相应值分别为89%和78%。
在ER入院时,主要创伤患者的FIB与快速可得的常规实验室参数如Hb和BE密切相关。这两个参数可能为识别有获得性低纤维蛋白原血症风险的主要创伤患者提供一种有见地且快速的工具。早期计算ISS可进一步提高预测这些患者FIB的能力。我们建议在创伤护理的初始阶段可根据床旁检测估算FIB。