Gonzalez Leslie, Cravoisy Aurélie, Barraud Damien, Conrad Marie, Nace Lionel, Lemarié Jérémie, Bollaert Pierre-Edouard, Gibot Sébastien
Crit Care. 2013 Jul 12;17(4):R140. doi: 10.1186/cc12819.
A rational use of antibiotics is of paramount importance in order to prevent the emergence of multidrug resistant bacteria that can lead to therapeutic impasse, especially in intensive care units (ICUs). A de-escalation strategy is therefore naturally advocated as part of better antibiotics usage. However, the clinical impact of such a strategy has not been widely studied. We aimed to assess the feasibility and the clinical impact of a de-escalation strategy in a medical ICU and to identify factors associated when de-escalation was possible.
We performed a retrospective study of patients hospitalized in a medical ICU over a period of six months. Independent factors associated with de-escalation and its clinical impact were assessed.
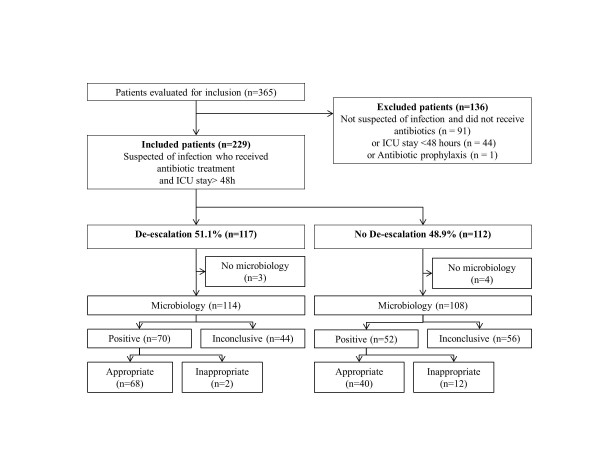
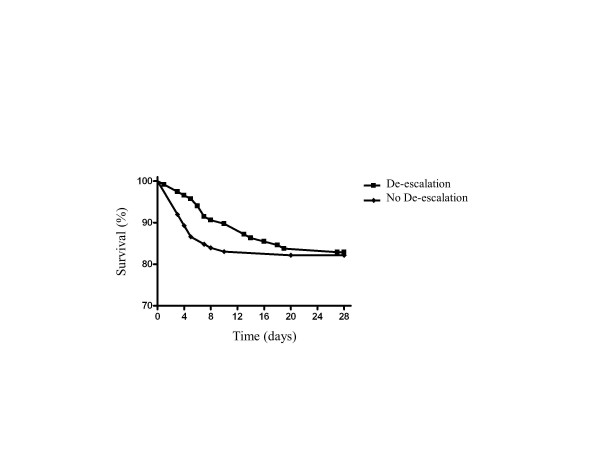
Two hundred and twenty-nine patients were included in the study. Antibiotics were de-escalated in 117 patients (51%). The appropriateness of initial antibiotic therapy was the only independent factor associated with the performance of de-escalation (OR = 2.9, 95% CI, 1.5-5.7; P = 0.002). By contrast, inadequacy of initial antibiotic therapy (OR = 0.1, 0.0 to 0.1, P <0.001) and the presence of multidrug resistant bacteria (OR = 0.2, 0.1 to 0.7, P = 0.006) prevented from de-escalation. There were no differences in terms of short (ICU) or long-term (at 1 year) mortality rates or any secondary criteria such as ICU length of stay, duration of antibiotic therapy, mechanical ventilation, incidence of ICU-acquired infection, or multi-drug resistant bacteria emergence.
De-escalation appears feasible in most cases without any obvious negative clinical impact in a medical ICU.
合理使用抗生素对于预防多重耐药菌的出现至关重要,多重耐药菌可导致治疗陷入困境,尤其是在重症监护病房(ICU)。因此,作为优化抗生素使用的一部分,自然提倡采用降阶梯策略。然而,这种策略的临床影响尚未得到广泛研究。我们旨在评估在医疗ICU中实施降阶梯策略的可行性和临床影响,并确定降阶梯可行时的相关因素。
我们对在医疗ICU住院6个月的患者进行了回顾性研究。评估了与降阶梯及其临床影响相关的独立因素。
229名患者纳入研究。117名患者(51%)实现了抗生素降阶梯。初始抗生素治疗的恰当性是与降阶梯实施相关的唯一独立因素(OR = 2.9,95%CI,1.5 - 5.7;P = 0.002)。相比之下,初始抗生素治疗不充分(OR = 0.1,0.0至0.1,P <0.001)和存在多重耐药菌(OR = 0.2,0.1至0.7,P = 0.006)阻碍了降阶梯。在短期(ICU)或长期(1年时)死亡率或任何次要标准方面,如ICU住院时间、抗生素治疗持续时间、机械通气、ICU获得性感染发生率或多重耐药菌出现情况,均无差异。
在医疗ICU中,大多数情况下降阶梯似乎可行,且无明显负面临床影响。