Chan Tiffany L, Goldstein Judith E, Massof Robert W
Lions Vision Research and Rehabilitation Center, Wilmer Eye Institute, The Johns Hopkins University School of Medicine, Baltimore, Maryland 21287, USA.
Optom Vis Sci. 2013 Aug;90(8):776-87. doi: 10.1097/OPX.0b013e31829d99d1.
To compare low-vision rehabilitation (LVR) clinicians' predictions of the probability of success of LVR with patients' self-reported outcomes after provision of usual outpatient LVR services and to determine if patients' traits influence clinician ratings.
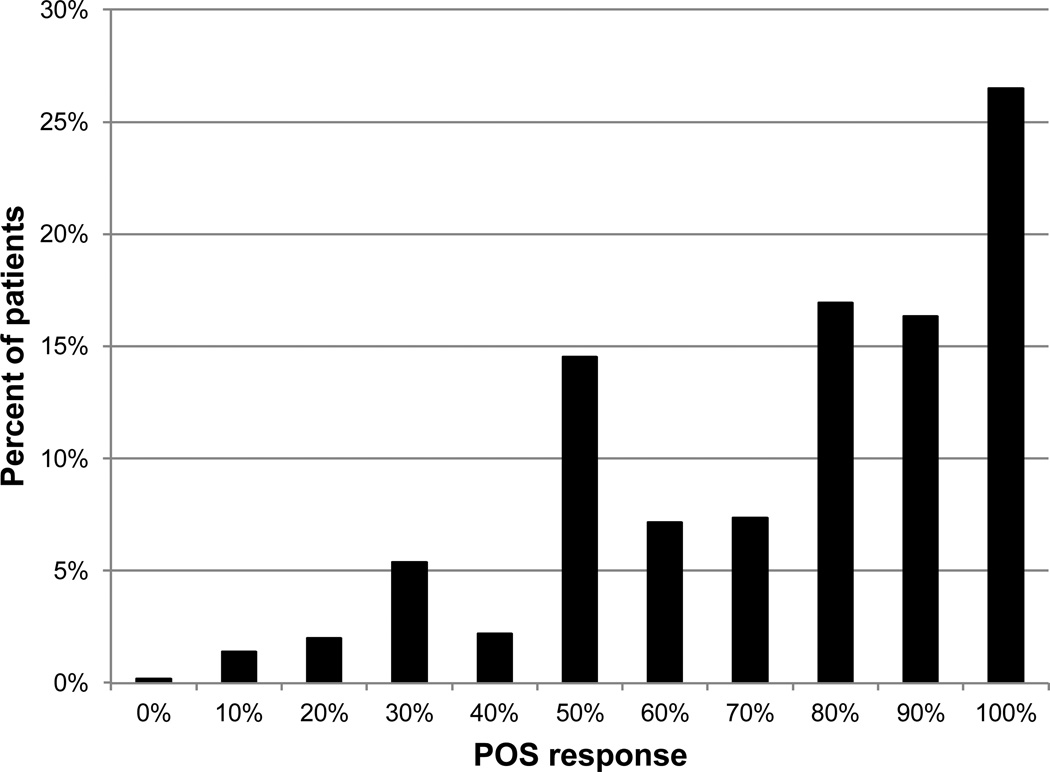
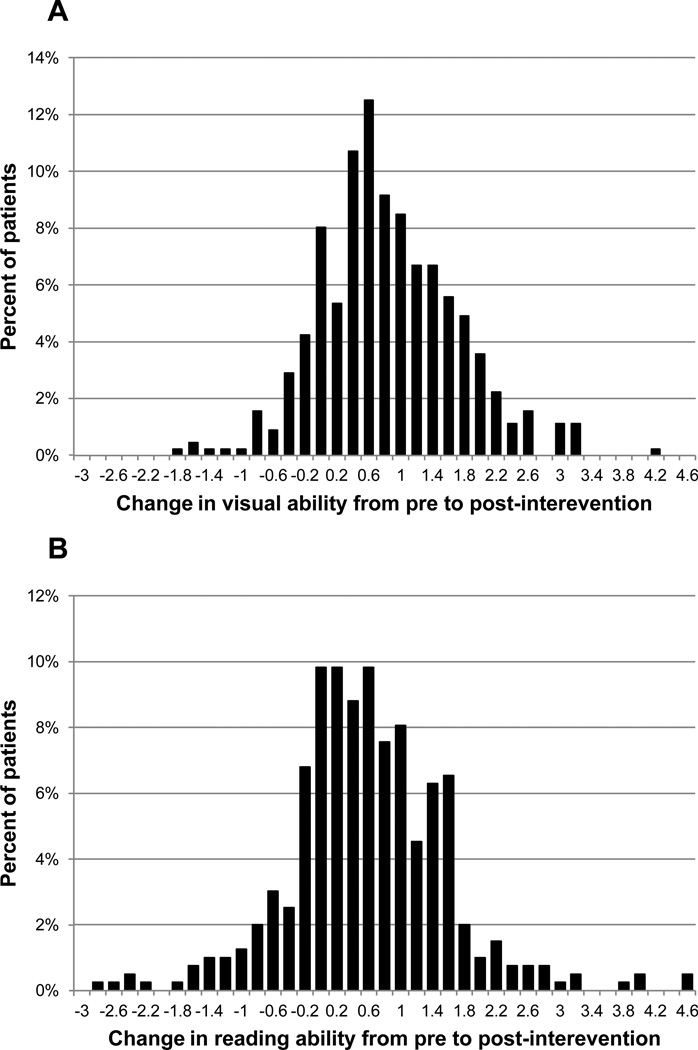
The Activity Inventory (AI), a self-report visual function questionnaire, was administered pre-and post-LVR to 316 low-vision patients served by 28 LVR centers that participated in a collaborative observational study. The physical component of the Short Form-36, Geriatric Depression Scale, and Telephone Interview for Cognitive Status were also administered pre-LVR to measure physical capability, depression, and cognitive status. After patient evaluation, 38 LVR clinicians estimated the probability of outcome success (POS) using their own criteria. The POS ratings and change in functional ability were used to assess the effects of patients' baseline traits on predicted outcomes.
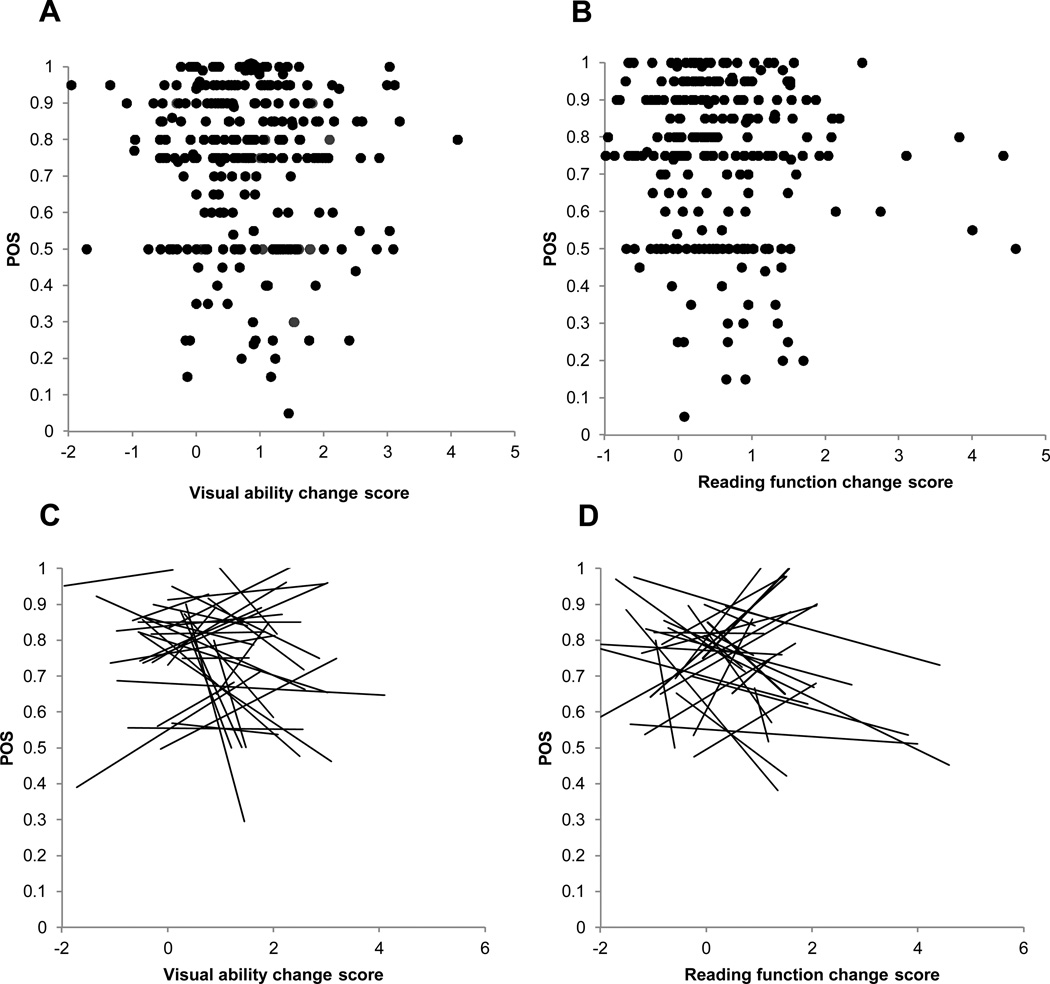
A regression analysis with a hierarchical random-effects model showed no relationship between LVR physician POS estimates and AI-based outcomes. In another analysis, kappa statistics were calculated to determine the probability of agreement between POS and AI-based outcomes for different outcome criteria. Across all comparisons, none of the kappa values were significantly different from 0, which indicates that the rate of agreement is equivalent to chance. In an exploratory analysis, hierarchical mixed-effects regression models show that POS ratings are associated with information about the patient's cognitive functioning and the combination of visual acuity and functional ability, as opposed to visual acuity or functional ability alone.
Clinicians' predictions of LVR outcomes seem to be influenced by knowledge of patients' cognitive functioning and the combination of visual acuity and functional ability-information clinicians acquire from the patient's history and examination. However, clinicians' predictions do not agree with observed changes in functional ability from the patient's perspective; they are no better than chance.
比较低视力康复(LVR)临床医生对LVR成功概率的预测与提供常规门诊LVR服务后患者自我报告的结果,并确定患者特征是否会影响临床医生的评分。
对参与一项协作观察性研究的28个LVR中心服务的316名低视力患者在LVR前后进行了自我报告视觉功能问卷《活动量表》(AI)的调查。在LVR前还进行了简短健康调查量表的身体成分、老年抑郁量表和认知状态电话访谈,以测量身体能力、抑郁和认知状态。在对患者进行评估后,38名LVR临床医生根据自己的标准估计结果成功概率(POS)。POS评分和功能能力变化用于评估患者基线特征对预测结果的影响。
采用分层随机效应模型的回归分析显示,LVR医生的POS估计与基于AI的结果之间没有关系。在另一项分析中,计算了kappa统计量,以确定不同结果标准下POS与基于AI的结果之间的一致概率。在所有比较中,没有一个kappa值与0有显著差异,这表明一致率等同于随机概率。在一项探索性分析中,分层混合效应回归模型显示,POS评分与患者认知功能信息以及视力和功能能力的组合相关,而不是单独的视力或功能能力。
临床医生对LVR结果的预测似乎受到患者认知功能知识以及视力和功能能力组合的影响,这些信息是临床医生从患者病史和检查中获得的。然而,从患者的角度来看,临床医生的预测与观察到的功能能力变化不一致;它们并不比随机猜测好。