Division of Infectious Diseases and International Health, Department of Medicine, Duke University Medical Center, Durham, North Carolina, USA.
PLoS Negl Trop Dis. 2013 Jul 18;7(7):e2324. doi: 10.1371/journal.pntd.0002324. Print 2013.
The syndrome of fever is a commonly presenting complaint among persons seeking healthcare in low-resource areas, yet the public health community has not approached fever in a comprehensive manner. In many areas, malaria is over-diagnosed, and patients without malaria have poor outcomes.
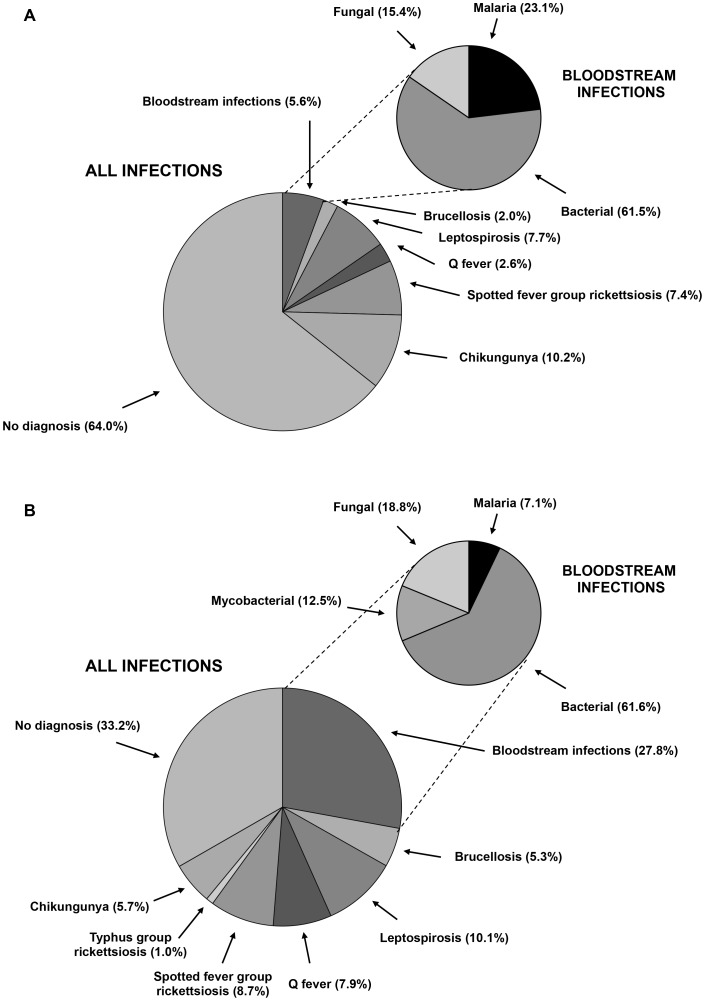
We prospectively studied a cohort of 870 pediatric and adult febrile admissions to two hospitals in northern Tanzania over the period of one year using conventional standard diagnostic tests to establish fever etiology. Malaria was the clinical diagnosis for 528 (60.7%), but was the actual cause of fever in only 14 (1.6%). By contrast, bacterial, mycobacterial, and fungal bloodstream infections accounted for 85 (9.8%), 14 (1.6%), and 25 (2.9%) febrile admissions, respectively. Acute bacterial zoonoses were identified among 118 (26.2%) of febrile admissions; 16 (13.6%) had brucellosis, 40 (33.9%) leptospirosis, 24 (20.3%) had Q fever, 36 (30.5%) had spotted fever group rickettsioses, and 2 (1.8%) had typhus group rickettsioses. In addition, 55 (7.9%) participants had a confirmed acute arbovirus infection, all due to chikungunya. No patient had a bacterial zoonosis or an arbovirus infection included in the admission differential diagnosis.
Malaria was uncommon and over-diagnosed, whereas invasive infections were underappreciated. Bacterial zoonoses and arbovirus infections were highly prevalent yet overlooked. An integrated approach to the syndrome of fever in resource-limited areas is needed to improve patient outcomes and to rationally target disease control efforts.
发热综合征是在资源匮乏地区寻求医疗保健的人群中常见的主诉,但公共卫生界尚未全面地处理发热问题。在许多地区,疟疾被过度诊断,而没有疟疾的患者则预后较差。
我们前瞻性地研究了坦桑尼亚北部两家医院的 870 名儿科和成年发热住院患者,使用常规标准诊断测试确定发热病因。528 例(60.7%)的临床诊断为疟疾,但实际上仅为 14 例(1.6%)发热的病因。相比之下,细菌、分枝杆菌和真菌感染引起的菌血症分别占发热住院患者的 85(9.8%)、14(1.6%)和 25(2.9%)。118 例(26.2%)发热患者中发现急性细菌性动物源性传染病;16 例(13.6%)患有布鲁氏菌病,40 例(33.9%)患有钩端螺旋体病,24 例(20.3%)患有 Q 热,36 例(30.5%)患有斑点热群立克次体病,2 例(1.8%)患有斑疹伤寒群立克次体病。此外,55 例(7.9%)患者有确诊的急性虫媒病毒感染,均由基孔肯雅热引起。入院鉴别诊断中没有患者患有细菌性动物源性传染病或虫媒病毒感染。
疟疾罕见且被过度诊断,而侵袭性感染则被低估。细菌性动物源性传染病和虫媒病毒感染非常普遍,但却被忽视了。在资源有限的地区,需要采用综合方法来处理发热综合征,以改善患者的预后,并合理地针对疾病控制工作。