Chekol Musse Tadesse, Sugerman David, Tayachew Adamu, Mekuria Zelalem, Tesfaye Neamin, Alemu Aynalem, Gashu Andargachew, Shura Wolde, Gonta Melaku, Agune Admikew, Hailemariam Aster, Assefa Yonas, Wossen Mesfin, Hassen Abdulhafiz, Michele Parsons, Silver Rachel, Delelegn Hulemenaw, Briana Lozano, Kasa Tesfu, Kebede Nigatu
Public Health Emergency Management Center, Ethiopian Public Health Institute, Addis Ababa, Ethiopia.
Aklilu Lemma Institute of Pathobiology, Addis Ababa University, Addis Ababa, Ethiopia.
Front Public Health. 2025 Jul 9;13:1549159. doi: 10.3389/fpubh.2025.1549159. eCollection 2025.
Viral respiratory pathogens have become the leading cause of acute undifferentiated febrile illness (AFI). We determined the fraction of AFI attributable to influenza and SARS-CoV-2 in Ethiopia, along with an understanding of their epidemiological characteristics.
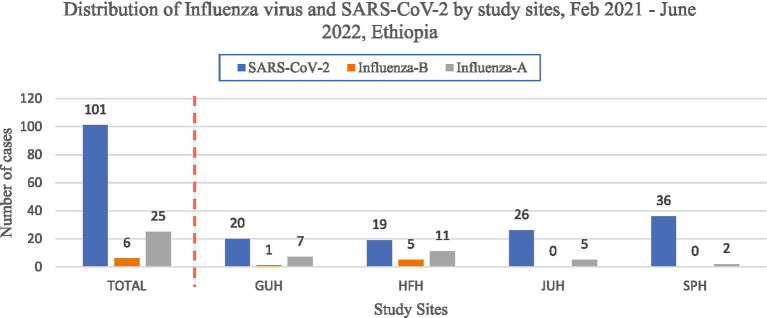
From February 2021 to June 2022, we enrolled patients meeting an AFI case definition (age >5 years with fever ≥38°C) who presented at one of four selected sentinel hospital sites in Jimma, Harari, Addis Ababa, and Gonder. Clinical and epidemiological information was collected, Nasopharyngeal swab samples were collected and analyzed using real-time PCR for respiratory viruses (influenza and SARS-CoV-2). A quasi-binomial regression model and multivariable regression were performed to compute fractions and establish associations with the agent detected.
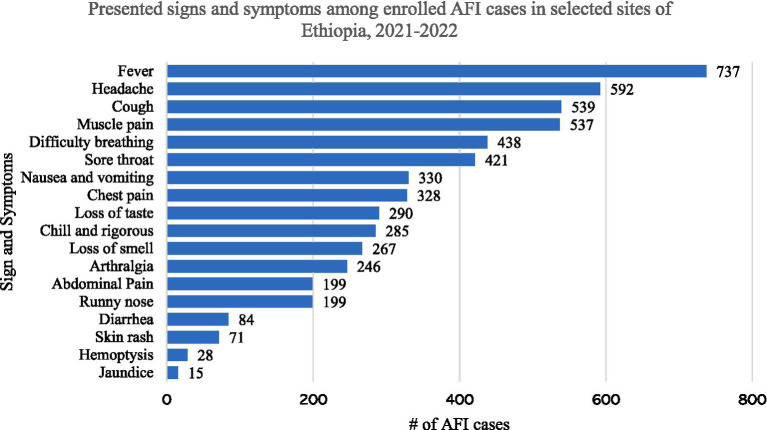
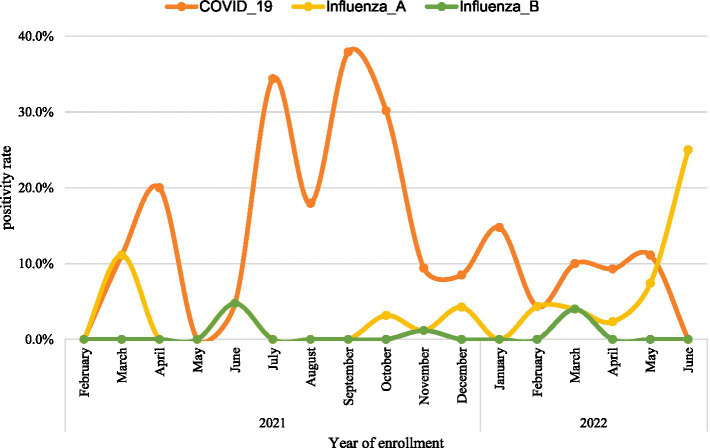
A total of 737 AFI cases were enrolled. The overall proportion of SARS-CoV-2, influenza A, and influenza B among AFI patients were 7.8, 1.9, and 0.5 per 100,000 population, respectively. Among the enrolled AFI cases tested for SARS-CoV-2 and Influenza virus, SARS-CoV-2 was the most detected pathogen with a positivity rate of 13.7% (95% CI:11.3-16.4), followed by influenza A and influenza B, which have a positivity rate of 3.3% (95% CI: 2.2-5.1) and 0.8% (95% CI:0.3-1.8), respectively. The positivity rate of SARS-CoV-2 peaked at 37.4% in September 2021. Per the multivariable analysis, cases ≥65 years of age were three [AOR = 3.3,95% CI:(1.9-5.7)] times more likely to be positive for SARS-CoV-2.
SARS-CoV-2 and influenza viruses were highly prevalent among AFI cases. The proportion of SARS-CoV-2 was higher among older adults. Further study is recommended to characterize influenza subtypes, SARS-CoV-2 variants and determine their attributable fraction among a broader panel of AFI-causing pathogens that contributes for guiding the proper diagnostics, treatment and surveillance measures.
病毒性呼吸道病原体已成为急性未分化发热性疾病(AFI)的主要病因。我们确定了埃塞俄比亚AFI中归因于流感和新冠病毒的比例,并了解了它们的流行病学特征。
2021年2月至2022年6月,我们纳入了符合AFI病例定义(年龄>5岁,发热≥38°C)且在吉姆马、哈拉里、亚的斯亚贝巴和贡德尔四个选定哨点医院之一就诊的患者。收集临床和流行病学信息,采集鼻咽拭子样本,并使用实时PCR检测呼吸道病毒(流感和新冠病毒)。进行了准二项回归模型和多变量回归分析,以计算比例并确定与检测到的病原体的关联。
共纳入737例AFI病例。AFI患者中新冠病毒、甲型流感和乙型流感的总体比例分别为每10万人7.8、1.9和0.5例。在接受新冠病毒和流感病毒检测的AFI病例中,新冠病毒是检测到最多的病原体,阳性率为13.7%(95%CI:11.3 - 16.4),其次是甲型流感和乙型流感,阳性率分别为3.3%(95%CI:2.2 - 5.1)和0.8%(95%CI:0.3 - 1.8)。新冠病毒的阳性率在2021年9月达到峰值37.4%。根据多变量分析,≥65岁的病例感染新冠病毒呈阳性的可能性是[调整后比值比(AOR)= 3.3,95%CI:(1.9 - 5.7)]三倍。
新冠病毒和流感病毒在AFI病例中高度流行。老年人中新冠病毒的比例更高。建议进一步研究以确定流感亚型、新冠病毒变体,并在更广泛的导致AFI的病原体中确定它们的归因比例,以指导适当的诊断、治疗和监测措施。