Department of Obstetrics and Gynecology, Cantonal Hospital, Frauenfeld, Switzerland.
J Gynecol Oncol. 2013 Jul;24(3):236-41. doi: 10.3802/jgo.2013.24.3.236. Epub 2013 Jul 4.
The malignant potential of intraepithelial neoplasia of the vulva and vagina after treatment is not well defined. Our objective was to examine risk factors for recurrence and invasive disease.
Four hundred sixty-four women with biopsy proven high-grade intraepithelial neoplasia of the vulva and vagina were identified in the electronic databases of four colposcopy clinics. Inclusion criteria were a follow-up of more than one year, no history of invasive cancer and no invasive cancer within the first year after initial treatment. We investigated the potential factors associated with recurrence and progression using a logistic regression analysis to estimate odds ratios (ORs) and 95% confidence intervals (CIs).
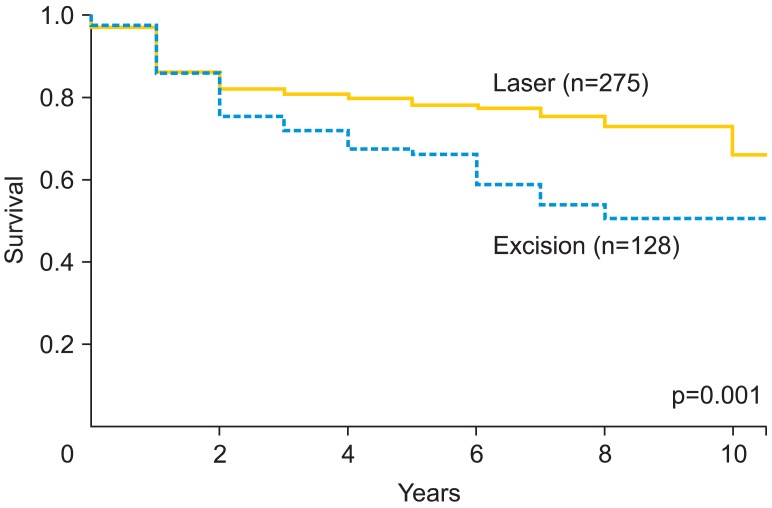
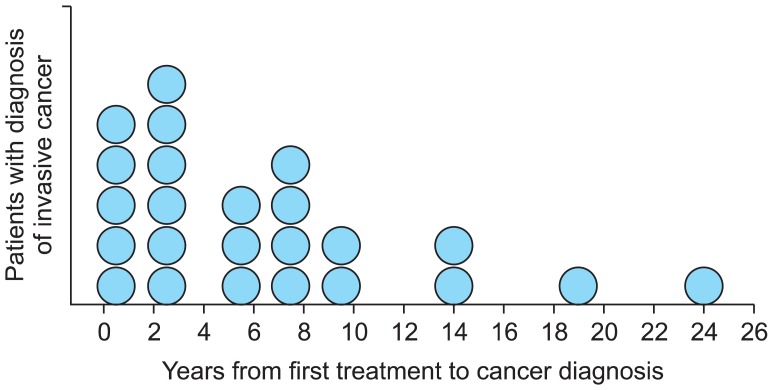
Of the 411 eligible patients, 123 patients (29.9%) recurred later than one year after initial treatment and 24 patients (5.8%) progressed to invasive disease. According to multivariate analyses, the risk factors associated with recurrence were multifocality (OR, 3.33; 95% CI, 2.02 to 5.51), immunosuppression (OR, 2.51; 95% CI, 1.09 to 5.81), excision as initial treatment (vs. laser evaporation; OR, 1.79; 95% CI, 1.11 to 2.91) and smoking (OR, 1.61; 95% CI, 1.02 to 2.55). Risk factors for progression to invasive disease were immunosuppression (OR, 4.00; 95% CI, 1.30 to 12.25), multifocality (OR, 3.05; 95% CI, 1.25 to 7.43) and smoking (OR, 2.97; 95% CI, 1.16 to 7.60), but not treatment modality.
Laser evaporation combined with extensive biopsy is at least as efficacious as initial treatment of intraepithelial neoplasia with excision. Smoking is a risk factor for both recurrence and progression to invasive disease. Hence, smoking cessation should be advised and maintaining a long follow-up period due to late relapses is necessary.
外阴和阴道上皮内瘤变(VIN 和 VaIN)经治疗后的恶性潜能尚不清楚。本研究旨在探讨其复发和浸润性疾病的危险因素。
在四家阴道镜诊所的电子数据库中,我们确定了 464 例经活检证实为外阴和阴道高级别上皮内瘤变的患者。纳入标准为随访时间超过 1 年,无浸润性癌病史,且在初始治疗后 1 年内无浸润性癌。我们使用逻辑回归分析来调查与复发和进展相关的潜在因素,以估计比值比(OR)和 95%置信区间(CI)。
在 411 例符合条件的患者中,123 例(29.9%)在初始治疗 1 年后复发,24 例(5.8%)进展为浸润性疾病。根据多变量分析,与复发相关的危险因素包括多发病灶(OR,3.33;95%CI,2.02 至 5.51)、免疫抑制(OR,2.51;95%CI,1.09 至 5.81)、初始治疗为切除术(vs. 激光蒸发术;OR,1.79;95%CI,1.11 至 2.91)和吸烟(OR,1.61;95%CI,1.02 至 2.55)。进展为浸润性疾病的危险因素包括免疫抑制(OR,4.00;95%CI,1.30 至 12.25)、多发病灶(OR,3.05;95%CI,1.25 至 7.43)和吸烟(OR,2.97;95%CI,1.16 至 7.60),但治疗方式不是危险因素。
激光蒸发术联合广泛活检与切除术治疗上皮内瘤变同样有效。吸烟是复发和进展为浸润性疾病的危险因素。因此,建议患者戒烟,并由于存在迟发性复发,应进行长期随访。