Department of Radiology, Memorial Sloan-Kettering Cancer Center, New York, NY, USA,
Ann Surg Oncol. 2013 Dec;20 Suppl 3(Suppl 3):S676-83. doi: 10.1245/s10434-013-3140-1. Epub 2013 Jul 30.
The objective of this work was to evaluate the feasibility of histopathological analysis of tissue extracted on multitined electrodes and assess whether tissue characteristics can be used as biomarkers of oncologic outcomes after lung tumor radiofrequency (RF) ablation.
Treatment-related data regarding RF ablation of lung malignancies at our institution was collected using a Health Insurance Portability and Accountability Act-compliant ablation database. Institutional review board waiver was obtained for this study. Immunohistochemical analysis of tissue extracted from the electrodes after lung tumor RF ablation was performed for proliferation (Ki-67) and apoptosis (caspase-3). Patient, tumor demographics, and ablation parameters were recorded. Local tumor progression-free survival (LPFS), disease-specific survival (DSS), and overall survival (OS) were assessed using Kaplan-Meier methodology. Multivariate analysis determined factors affecting these oncological outcomes.
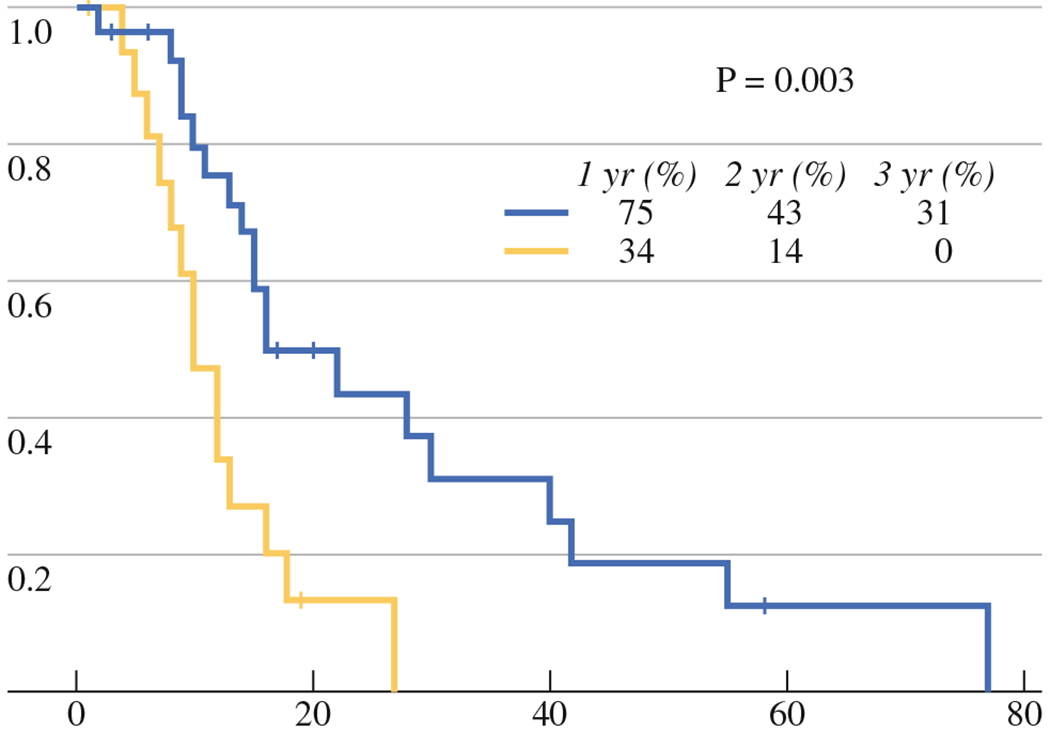
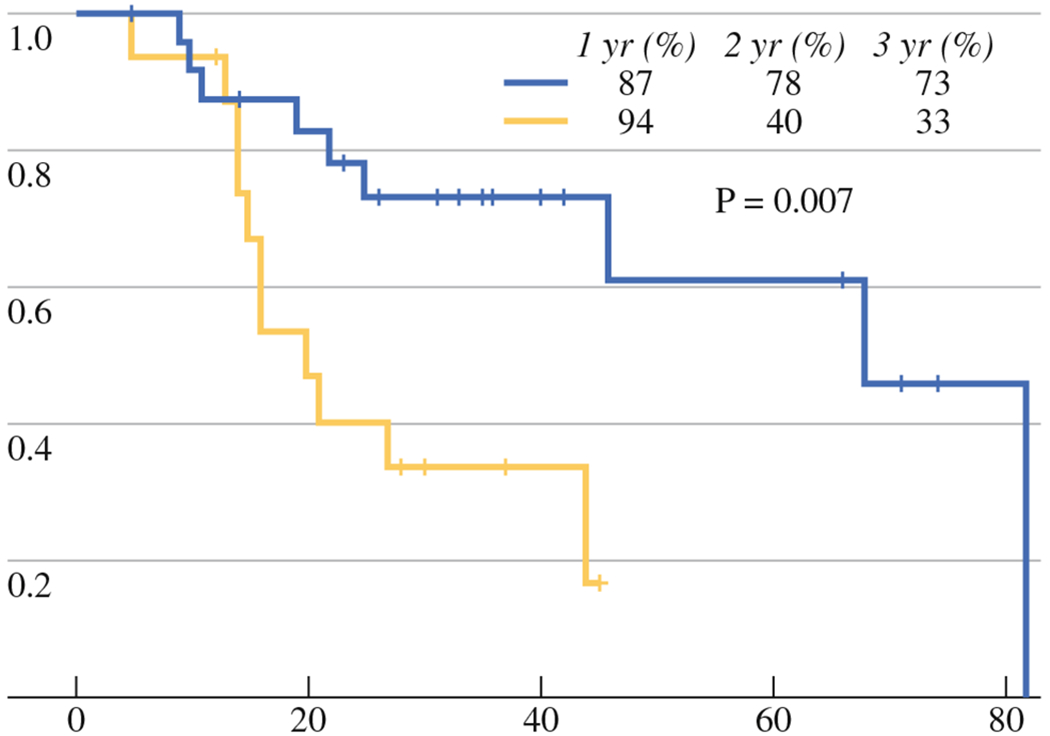
A total of 47 lung tumors in 42 patients were ablated; 30 specimens were classified as coagulation necrosis (CN) and 17 as Ki-67-positive (+) tumor cells (viable). Tumor sizes were similar in the CN and Ki-67+ groups (P = 0.32). Median LPFS was 10 versus 16 months for Ki-67+ and CN groups, and 1-year LPFS was 34 and 75 %, respectively (P = 0.003). Median OS was 20 and 46 months (P = 0.12), and median DSS was 20 and 68 months (P = 0.01) for the Ki-67 + and CN groups, respectively. Identification of Ki-67+ tumor cells more than tripled the risk of death from cancer [hazard ratio (HR) = 3.65; 95 % confidence interval (95 % CI), 1.34-9.95; P = 0.01] and tripled the risk of local tumor progression (LTP) (HR = 3.01; 95 % CI, 1.39-6.49; P = 0.005).
Ki-67+ tumor cells on the electrode after pulmonary tumor RF ablation is an independent predictor of LTP, shorter LPFS, and DSS.
本研究旨在评估从多齿电极提取的组织进行组织病理学分析的可行性,并评估组织特征是否可作为肺肿瘤射频 (RF) 消融后肿瘤学结果的生物标志物。
使用符合健康保险流通与责任法案 (HIPAA) 的消融数据库收集我院肺恶性肿瘤 RF 消融治疗相关数据。本研究获得机构审查委员会豁免。对肺肿瘤 RF 消融后从电极提取的组织进行增殖 (Ki-67) 和凋亡 (caspase-3) 的免疫组织化学分析。记录患者、肿瘤人口统计学和消融参数。采用 Kaplan-Meier 方法评估局部肿瘤无进展生存率 (LPFS)、疾病特异性生存率 (DSS) 和总生存率 (OS)。多变量分析确定影响这些肿瘤学结果的因素。
共对 42 例患者的 47 个肺肿瘤进行了消融;30 个标本分类为凝固性坏死 (CN),17 个标本为 Ki-67 阳性 (+) 肿瘤细胞 (存活)。CN 组和 Ki-67+组的肿瘤大小相似 (P = 0.32)。Ki-67+组和 CN 组的中位 LPFS 分别为 10 个月和 16 个月,1 年 LPFS 分别为 34%和 75% (P = 0.003)。Ki-67+组和 CN 组的中位 OS 分别为 20 个月和 46 个月 (P = 0.12),中位 DSS 分别为 20 个月和 68 个月 (P = 0.01)。Ki-67+肿瘤细胞的鉴定使癌症死亡风险增加两倍以上 (危险比[HR] = 3.65;95%置信区间[95%CI],1.34-9.95;P = 0.01),局部肿瘤进展 (LTP) 的风险增加两倍 (HR = 3.01;95%CI,1.39-6.49;P = 0.005)。
肺肿瘤 RF 消融后电极上的 Ki-67+肿瘤细胞是 LTP、LPFS 和 DSS 较短的独立预测因子。