International Centre for Circulatory Health, National Heart and Lung Institute, Imperial College London, , London, UK.
Heart. 2014 Mar;100(6):456-64. doi: 10.1136/heartjnl-2013-304262. Epub 2013 Jul 31.
Current European and American guidelines recommend the perioperative initiation of a course of β-blockers in those at risk of cardiac events undergoing high- or intermediate-risk surgery or vascular surgery. The Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography (DECREASE) family of trials, the bedrock of evidence for this, are no longer secure. We therefore conducted a meta-analysis of randomised controlled trials of β-blockade on perioperative mortality, non-fatal myocardial infarction, stroke and hypotension in non-cardiac surgery using the secure data.
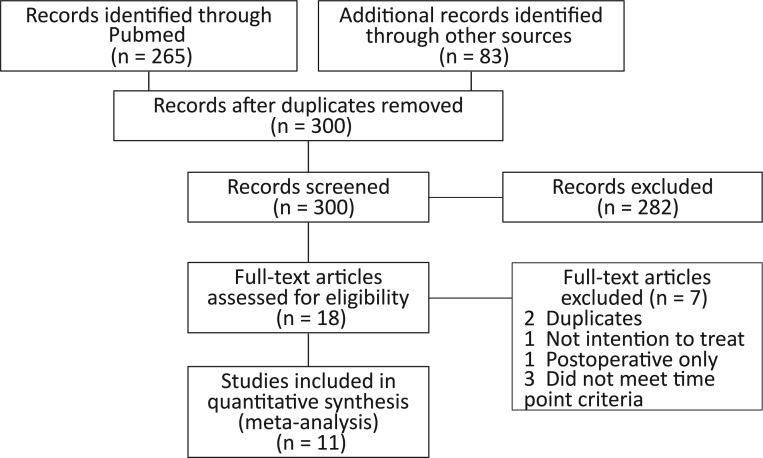
The randomised controlled trials of initiation of β-blockers before non-cardiac surgery were examined. Primary outcome was all-cause mortality at 30 days or at discharge. The DECREASE trials were separately analysed.
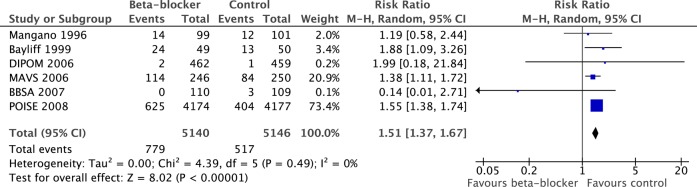
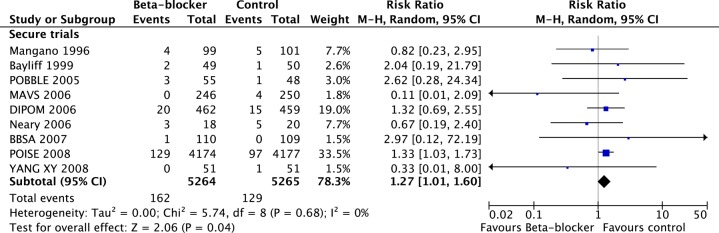
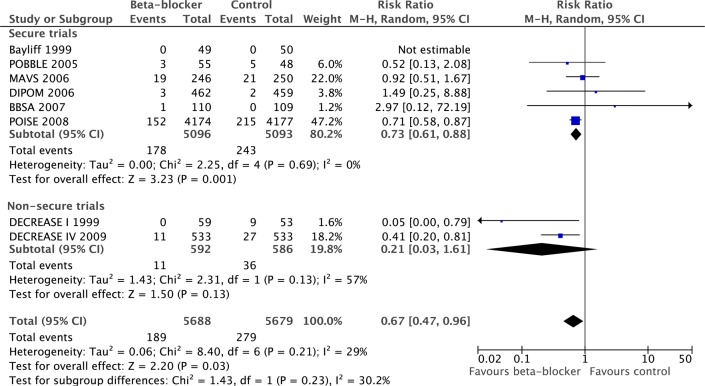
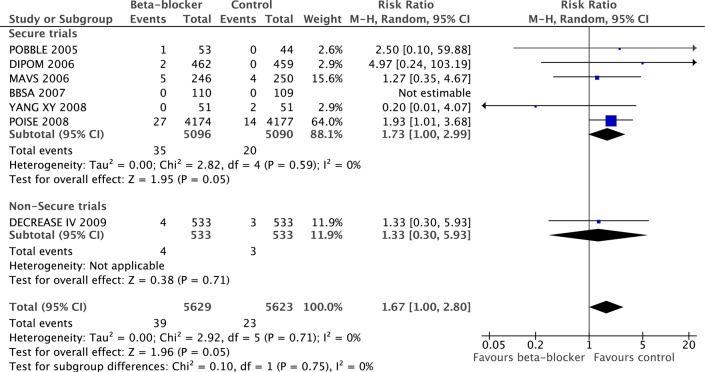
Nine secure trials totalling 10 529 patients, 291 of whom died, met the criteria. Initiation of a course of β-blockers before surgery caused a 27% risk increase in 30-day all-cause mortality (p=0.04). The DECREASE family of studies substantially contradict the meta-analysis of the secure trials on the effect of mortality (p=0.05 for divergence). In the secure trials, β-blockade reduced non-fatal myocardial infarction (RR 0.73, p=0.001) but increased stroke (RR 1.73, p=0.05) and hypotension (RR 1.51, p<0.00001). These results were dominated by one large trial.
Guideline bodies should retract their recommendations based on fictitious data without further delay. This should not be blocked by dispute over allocation of blame. The well-conducted trials indicate a statistically significant 27% increase in mortality from the initiation of perioperative β-blockade that guidelines currently recommend. Any remaining enthusiasts might best channel their energy into a further randomised trial which should be designed carefully and conducted honestly.
目前,欧美指南建议对有心脏事件风险的高危或中危手术或血管手术患者,在围手术期开始使用β受体阻滞剂。荷兰超声心动图心脏风险评估应用应激超声心动图(DECREASE)系列试验是支持这一建议的基石,但这些试验结果不再可靠。因此,我们使用可靠的数据,对围手术期使用β受体阻滞剂预防非心脏手术患者死亡、非致死性心肌梗死、卒中和低血压的随机对照试验进行了荟萃分析。
我们对非心脏手术前开始使用β受体阻滞剂的随机对照试验进行了研究。主要结局为 30 天或出院时的全因死亡率。单独分析了 DECREASE 试验。
共有 9 项可靠试验,总计 10529 例患者,其中 291 例死亡,符合纳入标准。术前开始使用β受体阻滞剂会使 30 天全因死亡率增加 27%(p=0.04)。DECREASE 系列研究与可靠试验的荟萃分析结果在死亡率方面存在显著差异(p=0.05,差异具有统计学意义)。在可靠的试验中,β受体阻滞剂减少了非致死性心肌梗死(RR 0.73,p=0.001),但增加了卒中(RR 1.73,p=0.05)和低血压(RR 1.51,p<0.00001)。这些结果主要来自一项大型试验。
指南制定机构应立即撤回基于虚假数据的推荐,而不应因责任归属的争议而受阻。精心设计、如实开展的进一步随机试验可能会让那些仍然热衷于β受体阻滞剂的人更好地发挥其能量。