Medical Care Research Unit, ScHARR, School of Health and Related Research (ScHARR), University of Sheffield, , Sheffield, UK.
BMJ Qual Saf. 2014 Jan;23(1):47-55. doi: 10.1136/bmjqs-2013-002003. Epub 2013 Jul 31.
Some emergency admissions can be avoided if acute exacerbations of health problems are managed by the range of health services providing emergency and urgent care.
To identify system-wide factors explaining variation in age sex adjusted admission rates for conditions rich in avoidable admissions.
National ecological study.
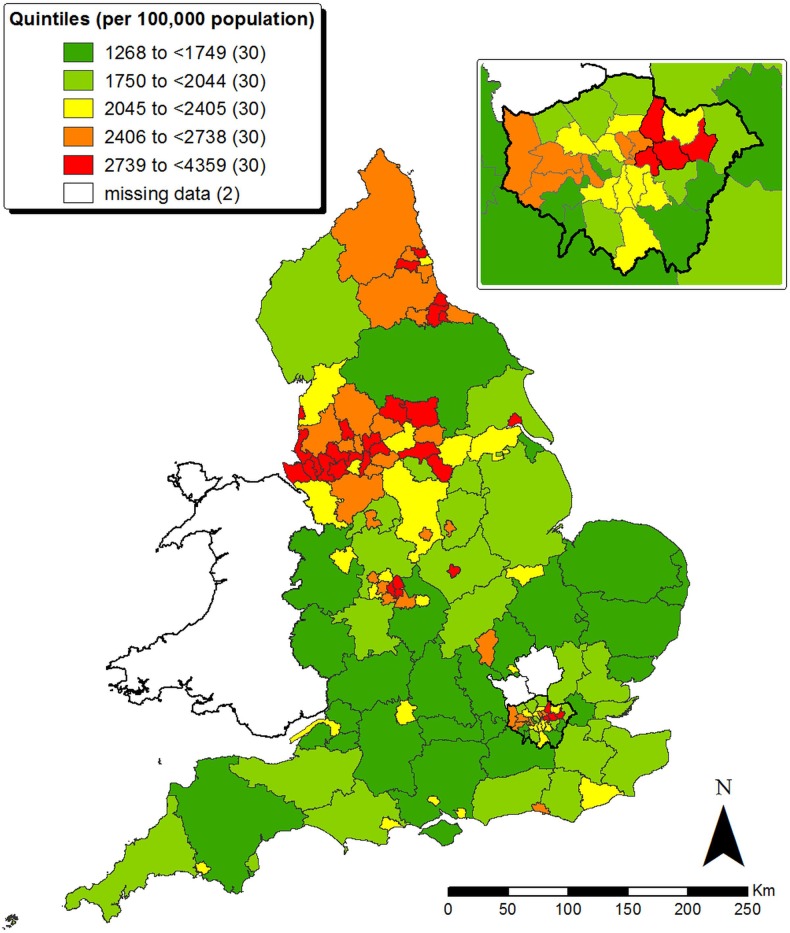
152 emergency and urgent care systems in England.
Hospital Episode Statistics data on emergency admissions were used to calculate an age sex adjusted admission rate for conditions rich in avoidable admissions for each emergency and urgent care system in England for 2008-2011.
There were 3 273 395 relevant admissions in 2008-2011, accounting for 22% of all emergency admissions. The mean age sex adjusted admission rate was 2258 per year per 100 000 population, with a 3.4-fold variation between systems (1268 and 4359). Factors beyond the control of health services explained the majority of variation: unemployment rates explained 72%, with urban/rural status explaining further variation (R(2)=75%). Factors related to emergency departments, hospitals, emergency ambulance services and general practice explained further variation (R(2)=85%): the attendance rate at emergency departments, percentage of emergency department attendances converted to admissions, percentage of emergency admissions staying less than a day, percentage of emergency ambulance calls not transported to hospital and perceived access to general practice within 48 h.
Interventions to reduce avoidable admissions should be targeted at deprived communities. Better use of emergency departments, ambulance services and primary care could further reduce avoidable emergency admissions.
如果健康问题的急性恶化由提供急诊和紧急护理的一系列卫生服务来管理,一些急诊入院是可以避免的。
确定解释可避免入院条件丰富的调整后年龄性别入院率差异的系统范围因素。
全国生态研究。
英格兰 152 个急诊和紧急护理系统。
使用医院入院统计数据计算 2008-2011 年英格兰每个急诊和紧急护理系统的可避免入院条件丰富的调整后年龄性别入院率。
2008-2011 年共有 3273395 例相关入院,占急诊入院的 22%。平均年龄性别调整入院率为每年每 10 万人 2258 例,系统间差异为 3.4 倍(1268 例至 4359 例)。超出卫生服务控制范围的因素解释了大部分差异:失业率解释了 72%,城市/农村状况进一步解释了差异(R²=75%)。与急诊部门、医院、急诊救护车服务和全科医生相关的因素进一步解释了差异(R²=85%):急诊部门就诊率、急诊部门就诊转换为入院的比例、急诊入院不足一天的比例、救护车呼叫未送往医院的比例以及在 48 小时内获得全科医生治疗的感知机会。
减少可避免入院的干预措施应针对贫困社区。更好地利用急诊部门、救护车服务和初级保健可以进一步减少可避免的急诊入院。