Université Lyon1, CNRS UMR 5558, Villeurbanne, F-69622, France.
BMC Infect Dis. 2013 Aug 1;13:359. doi: 10.1186/1471-2334-13-359.
Necrotizing pneumonia attributed to Panton-Valentine leukocidin-positive Staphylococcus aureus has mainly been reported in otherwise healthy children and young adults, with a high mortality rate. Erythroderma, airway bleeding, and leukopenia have been shown to be predictive of mortality. The objectives of this study were to define the characteristics of patients with severe leukopenia at 48-h hospitalization and to update our data regarding mortality predicting factors in a larger population than we had previously described.
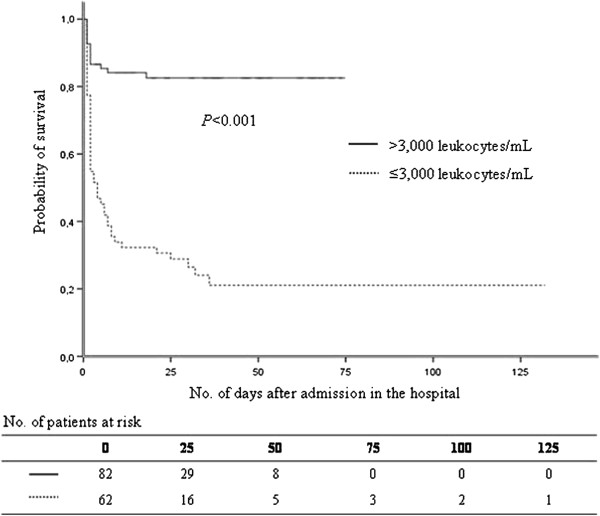
It was designed as a case-case study nested in a cohort study. A total of 148 cases of community-acquired, necrotizing pneumonia were included. The following data were collected: basic demographic information, medical history, signs and symptoms, radiological findings and laboratory results during the first 48 h of hospitalization. The study population was divided into 2 groups: (1) with severe leukopenia (leukocyte count ≤3,000 leukocytes/mL, n=62) and (2) without severe leukopenia (>3,000 leukocytes/mL, n=86).
Median age was 22 years, and the male-to-female gender ratio was 1.5. The overall in-hospital mortality rate was 41.2%. Death occurred in 75.8% of severe leukopenia cases with median survival time of 4 days, and in 16.3% of cases with leukocyte count >3,000/mL (P<0.001). Multivariate analysis indicated that the factors associated with severe leukopenia were influenza-like illness (adjusted odds ratio (aOR) 4.45, 95% CI (95% confidence interval) 1.67-11.88, P=0.003), airway bleeding (aOR 4.53, 95% CI 1.85-11.13, P=0.001) and age over 30 years (aOR 2.69, 95% CI 1.08-6.68, P=0.033). A personal history of furuncles appeared to be protective (OR 0.11, 95% CI 0.01-0.96, P=0.046).
S. aureus-necrotizing pneumonia is still an extremely severe disease in patients with severe leukopenia. Some factors could distinguish these patients, allowing better initial identification to initiate adapted, rapid administration of appropriate therapy.
由携带潘顿-瓦伦丁杀白细胞素的金黄色葡萄球菌引起的坏死性肺炎主要发生在其他健康的儿童和年轻人中,死亡率很高。红皮病、气道出血和白细胞减少已被证明是死亡的预测因素。本研究的目的是定义在入院 48 小时内严重白细胞减少的患者特征,并在比我们之前描述的更大的人群中更新我们关于死亡率预测因素的数据。
这是一项嵌套在队列研究中的病例对照研究。共纳入 148 例社区获得性坏死性肺炎患者。收集了以下数据:基本人口统计学信息、病史、症状和体征、住院后前 48 小时的影像学和实验室结果。研究人群分为两组:(1)严重白细胞减少组(白细胞计数≤3000 个/毫升,n=62)和(2)无严重白细胞减少组(白细胞计数>3000 个/毫升,n=86)。
中位年龄为 22 岁,男女比例为 1.5。总的院内死亡率为 41.2%。严重白细胞减少组死亡 75.8%,中位生存时间为 4 天,白细胞计数>3000 个/毫升的患者死亡率为 16.3%(P<0.001)。多变量分析表明,流感样疾病(调整后的优势比(aOR)4.45,95%可信区间(95%置信区间)1.67-11.88,P=0.003)、气道出血(aOR 4.53,95%CI 1.85-11.13,P=0.001)和年龄大于 30 岁(aOR 2.69,95%CI 1.08-6.68,P=0.033)与严重白细胞减少相关。个人疖病史似乎有保护作用(OR 0.11,95%CI 0.01-0.96,P=0.046)。
金黄色葡萄球菌坏死性肺炎在严重白细胞减少的患者中仍然是一种极其严重的疾病。一些因素可以区分这些患者,从而更好地进行初始识别,快速启动适当的治疗。