INSERM, U1018, Epidemiology of HIV and STI; University Paris-Sud 11, Le Kremlin-Bicêtre, France.
PLoS One. 2013 Aug 1;8(8):e71473. doi: 10.1371/journal.pone.0071473. Print 2013.
Guidelines for initiating HIV treatment are regularly revised. We explored how physicians in France have applied these evolving guidelines for ART initiation over the last decade in two different situations: chronic (CHI) and primary HIV-1 infection (PHI), since specific recommendations for PHI are also provided in France.
Data came from the ANRS PRIMO (1267 patients enrolled during PHI in 1996-2010) and COPANA (800 subjects enrolled at HIV diagnosis in 2004-2008) cohorts. We defined as guidelines-inconsistent during PHI and CHI, patients meeting criteria for ART initiation and not treated in the following month and during the next 6 months, respectively.
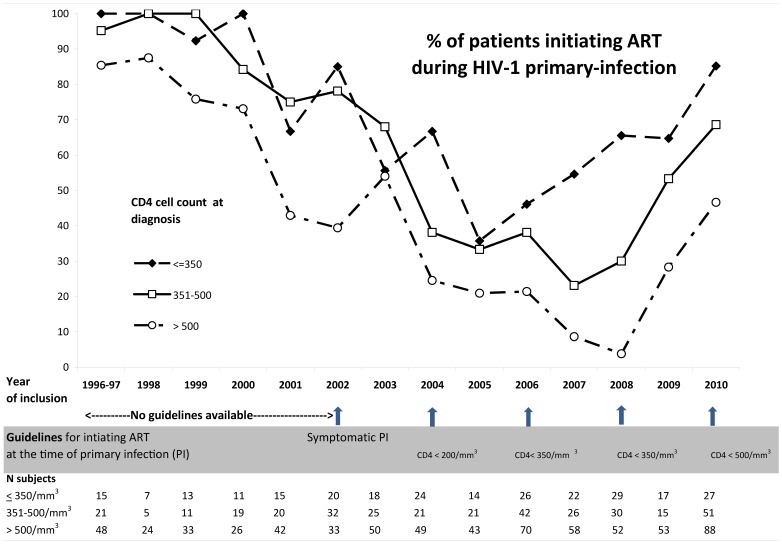
ART initiation during PHI dramatically decreased from 91% of patients in 1996-99 to 22% in 2007 and increased to 60% in 2010, following changes in recommendations. In 2007, however, after the CD4 count threshold was raised to 350 cells/mm(3) in 2006, only 55% of the patients with CD4≤350 were treated and 66% in 2008. During CHI, ART was more frequently initiated in patients who met the criteria at entry (96%) than during follow-up: 83% when recommendation to treat was 200 and 73% when it was 350 cells/mm(3). Independent risk factors for not being treated during CHI despite meeting the criteria were lower viral load, lower educational level, and poorer living conditions.
HIV ART initiation guidelines are largely followed by practitioners in France. What can still be improved, however, is time to treat when CD4 cell counts reach the threshold to treat. Risk factors for lack of timely treatment highlight the need to understand better how patients' living conditions and physicians' perceptions influence the decision to initiate treatment.
艾滋病病毒治疗指南经常修订。我们探索了法国医生在过去十年中在两种不同情况下如何应用这些不断变化的抗逆转录病毒治疗(ART)启动指南:慢性(CHI)和原发性 HIV-1 感染(PHI),因为法国也为 PHI 提供了具体的建议。
数据来自于 ANRS PRIMO(1996-2010 年期间 PHI 期间纳入的 1267 名患者)和 COPANA(2004-2008 年 HIV 诊断时纳入的 800 名患者)队列。我们将 PHI 和 CHI 期间符合 ART 启动标准但在下一个月和接下来的 6 个月内未接受治疗的患者定义为不符合指南。
PHI 期间的 ART 启动率从 1996-99 年的 91%急剧下降到 2007 年的 22%,并在 2010 年增加到 60%,这是由于建议的变化。然而,在 2006 年 CD4 计数阈值提高到 350 个细胞/mm³后,2007 年只有 55%的 CD4≤350 患者接受了治疗,2008 年为 66%。在 CHI 期间,符合标准的患者更常开始接受 ART(96%),而不是在随访期间:当治疗建议为 200 个时为 83%,当建议为 350 个细胞/mm³时为 73%。尽管符合标准,但在 CHI 期间未接受治疗的独立危险因素是病毒载量较低、教育程度较低和生活条件较差。
法国的医生在很大程度上遵循了 HIV ART 启动指南。然而,仍有待改进的是,当 CD4 细胞计数达到治疗阈值时,治疗的时间。缺乏及时治疗的危险因素突出表明,需要更好地了解患者的生活条件和医生的看法如何影响启动治疗的决策。