Dragovic Gordana, Smith Colette J, Jevtovic Djordje, Dimitrijevic Bozana, Kusic Jovana, Youle Mike, Johnson Margaret A
Department of Pharmacology, Clinical Pharmacology and Toxicology, School of Medicine, University of Belgrade, Belgrade, Serbia.
UCL Research Department of Infection and Population Health, Royal Free Campus, 1st Floor, Rowland Hill Street, London, NW3 2PF, UK.
BMC Infect Dis. 2016 Mar 3;16:106. doi: 10.1186/s12879-016-1443-0.
The range of combination antiretroviral therapy (cART) regimens available in many middle-income countries differs from those suggested in international HIV treatment guidelines. We compared first-line cART regimens, timing of initiation and treatment outcomes in a middle income setting (HIV Centre, Belgrade, Serbia - HCB) with a high-income country (Royal Free London Hospital, UK - RFH).
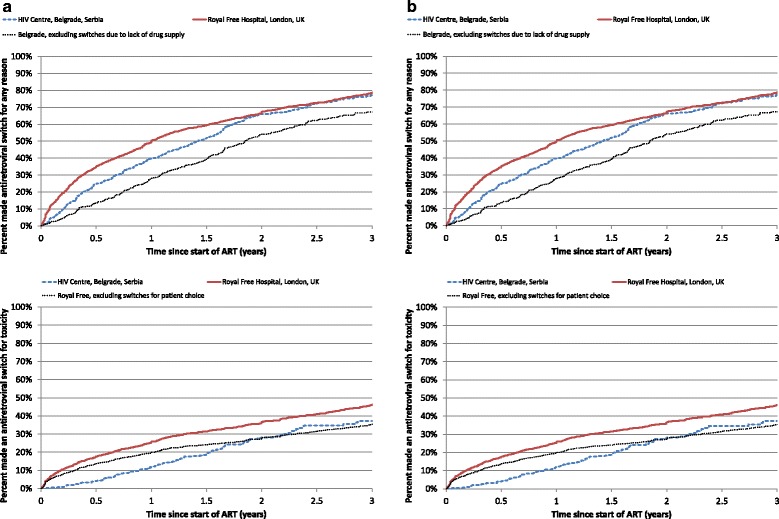
All antiretroviral-naïve HIV-positive individuals from HCB and RFH starting cART between 2003 and 2012 were included. 12-month viral load and CD4 count responses were compared, considering the first available measurement 12-24 months post-cART. The percentage that had made an antiretroviral switch for any reason, or for toxicity and the percentage that had died by 36 months (the latest time at which sufficient numbers remained under follow-up) were investigated using standard survival methods.
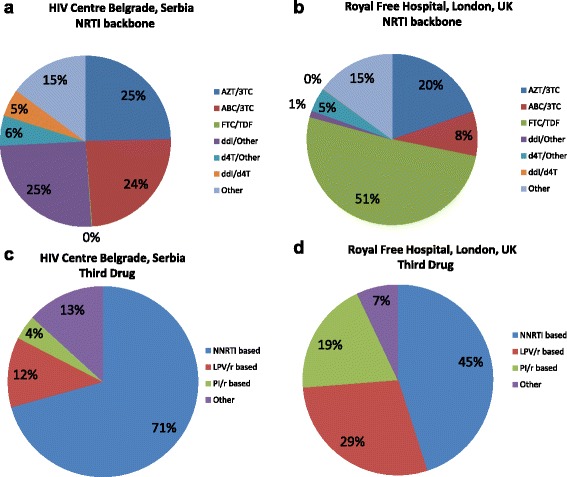
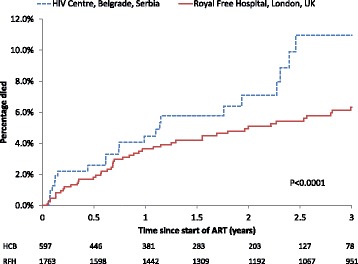
361/597 (61 %) of individuals initiating cART at HCB had a prior AIDS diagnosis, compared to 337/1763 (19 %) at RFH. Median pre-ART CD4 counts were 177 and 238 cells/mm(3) respectively (p < 0.0001). The most frequently prescribed antiretrovirals were zidovudine with lamivudine (149; 25 %) and efavirenz [329, 55 %] at HCB and emtricitabine with tenofovir (899; 51 %) and efavirenz [681, 39 %] at RFH. At HCB, a median of 2 CD4 count measurements in the first year of cART were taken, compared to 5 at RFH (p < 0.0001). Median (IQR) CD4 cell increase after 12 months was +211 (+86, +359) and +212 (+105, +318) respectively. 287 (48 %) individuals from HCB and 1452 (82 %) from RFH had an available viral load measurement, of which 271 (94 %) and 1280 (88 %) were <400 copies/mL (p < 0.0001). After 36 months, comparable percentages had made at least one antiretroviral switch (77 % HCB vs. 78 % RFH; p = 0.23). However, switches for toxicity/patient choice were more common at RFH. After 12 and 36 months of cART 3 % and 8 % of individuals died at HCB, versus 2 % and 4 % at RFH (p < 0.0001).
In middle-income countries, cART is usually started at an advanced stage of HIV disease, resulting in higher mortality rates than in high income countries, supporting improved testing campaigns for early detection of HIV infection and early introduction of newer cART regimens.
许多中等收入国家可用的联合抗逆转录病毒疗法(cART)方案与国际艾滋病治疗指南中建议的方案不同。我们比较了一个中等收入地区(塞尔维亚贝尔格莱德艾滋病中心 - HCB)和一个高收入国家(英国伦敦皇家自由医院 - RFH)的一线cART方案、开始治疗的时间以及治疗结果。
纳入了2003年至2012年间在HCB和RFH开始接受cART治疗的所有初治HIV阳性个体。比较了cART治疗12 - 24个月后的首次可用测量值的12个月病毒载量和CD4细胞计数反应。使用标准生存方法调查了因任何原因或因毒性而更换抗逆转录病毒药物的百分比以及36个月时(随访中仍有足够数量个体的最晚时间)死亡的百分比。
在HCB开始接受cART治疗的个体中,361/597(61%)曾有艾滋病诊断,而在RFH这一比例为337/1763(19%)。ART前CD4细胞计数中位数分别为177和238个细胞/mm³(p < 0.0001)。HCB最常开具的抗逆转录病毒药物是齐多夫定与拉米夫定(149例;25%)和依非韦伦[329例,55%],而RFH是恩曲他滨与替诺福韦(899例;51%)和依非韦伦[681例,39%]。在HCB,cART治疗第一年CD4细胞计数测量的中位数为2次,而RFH为5次(p < 0.0001)。12个月后CD4细胞增加的中位数(IQR)分别为+211(+86,+359)和+212(+105,+318)。HCB有287例(48%)个体和RFH有1452例(82%)个体有可用的病毒载量测量值,其中271例(94%)和1280例(88%)<400拷贝/mL(p < 0.0001)。36个月后,进行至少一次抗逆转录病毒药物更换的百分比相当(HCB为77%,RFH为78%;p = 0.23)。然而,因毒性/患者选择而更换药物在RFH更常见。cART治疗12个月和36个月后,HCB分别有3%和8%的个体死亡,而RFH分别为2%和4%(p < 0.0001)。
在中等收入国家中HIV疾病通常在晚期开始cART治疗,导致死亡率高于高收入国家,这支持加强检测活动以早期发现HIV感染并尽早引入更新的cART方案。