Sánchez Manuel, García-de-Lorenzo Abelardo, Herrero Eva, Lopez Teresa, Galvan Beatriz, Asensio María, Cachafeiro Lucia, Casado Cesar
Crit Care. 2013 Aug 15;17(4):R176. doi: 10.1186/cc12855.
The use of urinary output and vital signs to guide initial burn resuscitation may lead to suboptimal resuscitation. Invasive hemodynamic monitoring may result in over-resuscitation. This study aimed to evaluate the results of a goal-directed burn resuscitation protocol that used standard measures of mean arterial pressure (MAP) and urine output, plus transpulmonary thermodilution (TPTD) and lactate levels to adjust fluid therapy to achieve a minimum level of preload to allow for sufficient vital organ perfusion.
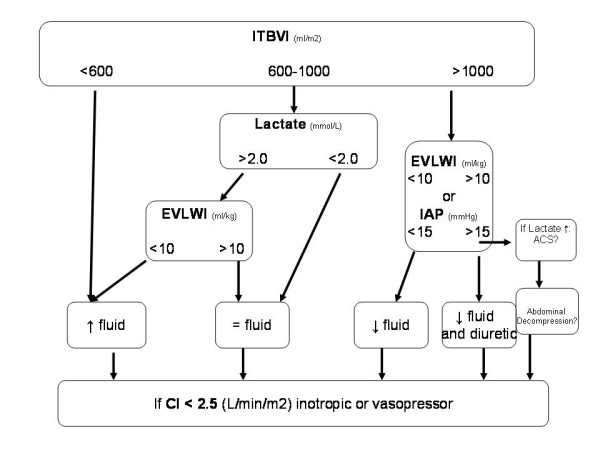
We conducted a three-year prospective cohort study of 132 consecutive critically burned patients. These patients underwent resuscitation guided by MAP (>65 mmHg), urinary output (0.5 to 1 ml/kg), TPTD and lactate levels. Fluid therapy was adjusted to achieve a cardiac index (CI) >2.5 L/minute/m² and an intrathoracic blood volume index (ITBVI) >600 ml/m2, and to optimize lactate levels. Statistical analysis was performed using mixed models. We also used Pearson or Spearman methods and the Mann-Whitney U-test.
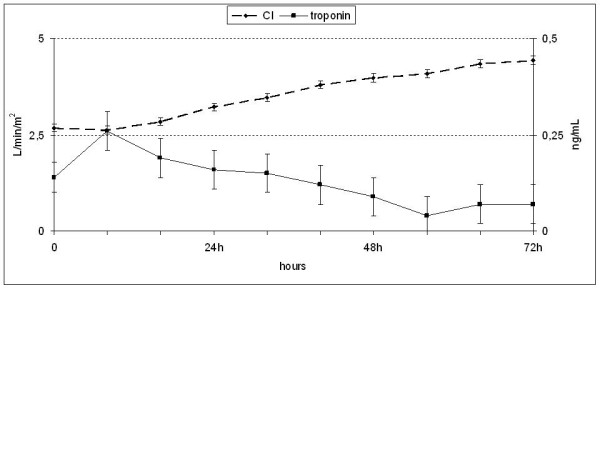
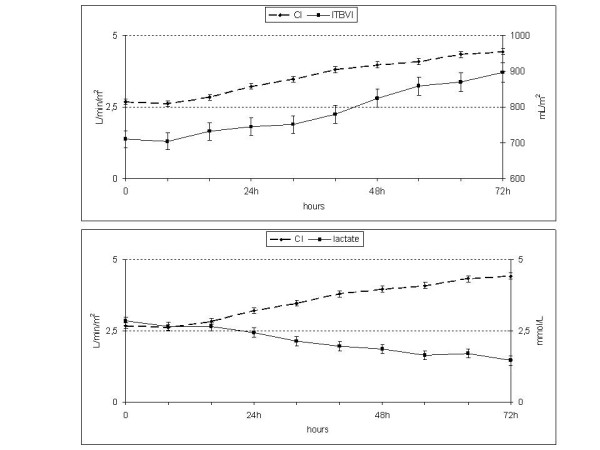
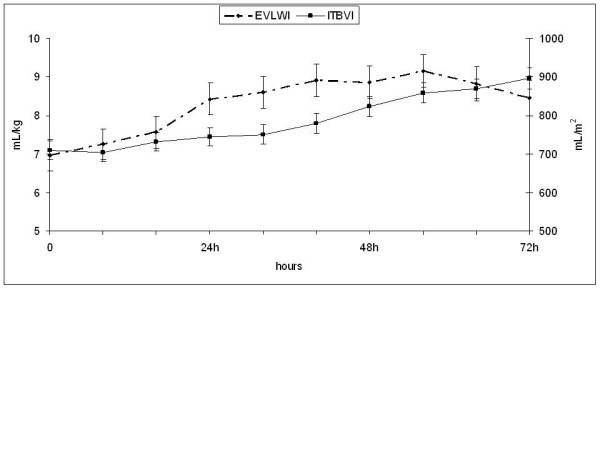
A total of 98 men and 34 women (mean age, 48 ± 18 years) was studied. The mean total body surface area (TBSA) burned was 35% ± 22%. During the early resuscitation phase, lactate levels were elevated (2.58 ± 2.05 mmol/L) and TPTD showed initial hypovolemia by the CI (2.68 ± 1.06 L/minute/m²) and the ITBVI (709 ± 254 mL/m²). At 24 to 32 hours, the CI and lactic levels were normalized, although the ITBVI remained below the normal range (744 ± 276 ml/m²). The mean fluid rate required to achieve protocol targets in the first 8 hours was 4.05 ml/kg/TBSA burned, which slightly increased in the next 16 hours. Patients with a urine output greater than or less than 0.5 ml/kg/hour did not show differences in heart rate, mean arterial pressure, CI, ITBVI or lactate levels.
Initial hypovolemia may be detected by TPTD monitoring during the early resuscitation phase. This hypovolemia might not be reflected by blood pressure and hourly urine output. An adequate CI and tissue perfusion can be achieved with below-normal levels of preload. Early resuscitation guided by lactate levels and below-normal preload volume targets appears safe and avoids unnecessary fluid input.
使用尿量和生命体征来指导初始烧伤复苏可能导致复苏效果欠佳。有创血流动力学监测可能会导致过度复苏。本研究旨在评估一种目标导向性烧伤复苏方案的效果,该方案使用平均动脉压(MAP)和尿量的标准测量值,加上经肺热稀释法(TPTD)和乳酸水平来调整液体治疗,以达到最低的前负荷水平,从而实现重要生命器官的充分灌注。
我们对132例连续的严重烧伤患者进行了为期三年的前瞻性队列研究。这些患者在MAP(>65 mmHg)、尿量(0.5至1 ml/kg)、TPTD和乳酸水平的指导下进行复苏。调整液体治疗以实现心脏指数(CI)>2.5 L/分钟/平方米和胸腔内血容量指数(ITBVI)>600 ml/m²,并优化乳酸水平。使用混合模型进行统计分析。我们还使用了Pearson或Spearman方法以及Mann-Whitney U检验。
共研究了98名男性和34名女性(平均年龄,48±18岁)。平均烧伤总面积(TBSA)为35%±22%。在早期复苏阶段,乳酸水平升高(2.58±2.05 mmol/L),TPTD显示CI(2.68±1.06 L/分钟/平方米)和ITBVI(709±254 mL/m²)存在初始血容量不足。在24至32小时,CI和乳酸水平恢复正常,尽管ITBVI仍低于正常范围(744±276 ml/m²)。在最初8小时内达到方案目标所需的平均液体输注速率为4.05 ml/kg/烧伤TBSA,在接下来的16小时内略有增加。尿量大于或小于0.5 ml/kg/小时的患者在心率、平均动脉压、CI、ITBVI或乳酸水平方面没有差异。
在早期复苏阶段,通过TPTD监测可能检测到初始血容量不足。这种血容量不足可能不会通过血压和每小时尿量反映出来。在低于正常水平的前负荷下可以实现足够的CI和组织灌注。以乳酸水平和低于正常的前负荷量目标为指导的早期复苏似乎是安全的,并且可以避免不必要的液体输入。