Shriners Hospitals for Children, 815 Market Street, Galveston, TX 77550, USA.
Crit Care. 2011;15(2):R118. doi: 10.1186/cc10147. Epub 2011 Apr 21.
Monitoring of hemodynamic and volumetric parameters after severe burns is of critical importance. Pulmonary artery catheters, however, have been associated with many risks. Our aim was to show the feasibility of continuous monitoring with minimally invasive transpulmonary thermodilution (TPTD) in severely burned pediatric patients.
This prospective cohort study was conducted in patients with severe burns over 40% of the total body surface area (TBSA) who were admitted to the hospital within 96 hours after sustaining the injury. TPTD measurements were performed using the PiCCO system (Pulsion Medical Systems, Munich, Germany). Cardiac Index (CI), Intrathoracic Blood Volume Index (ITBVI) (Stewart-Hamilton equation), Extravascular Lung Water Index (EVLWI) and Systemic Vascular Resistance Index (SVRI) measurements were recorded twice daily. Statistical analysis was performed using one-way repeated measures analysis of variance with the post hoc Bonferroni test for intra- and intergroup comparisons.
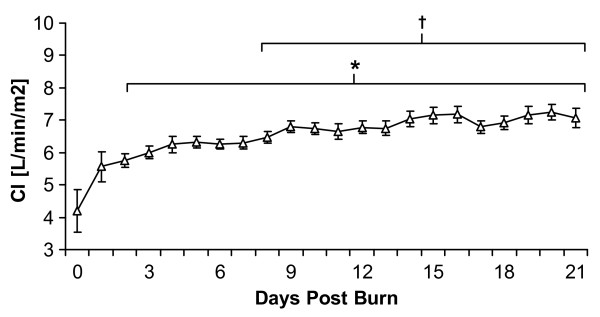
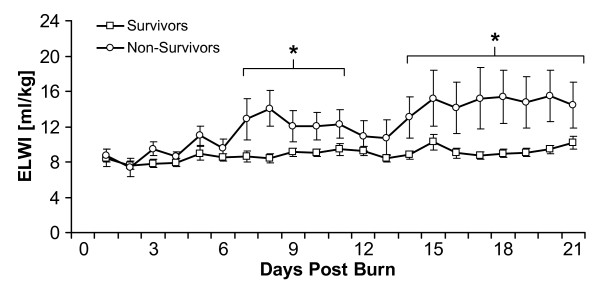
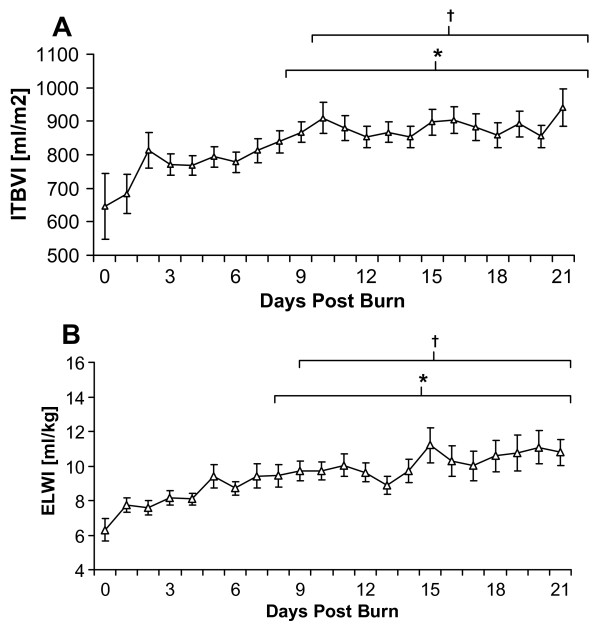
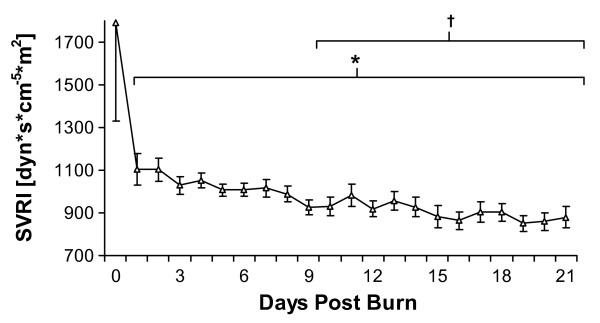
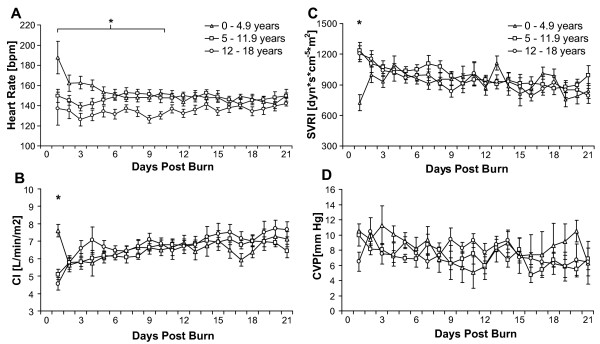
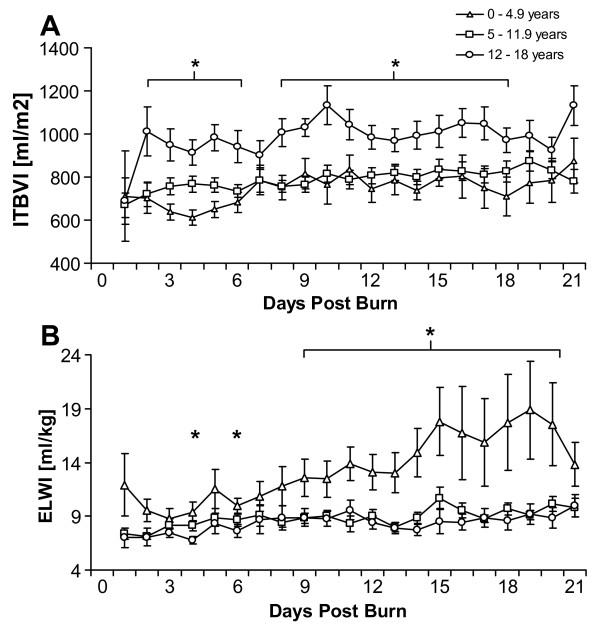
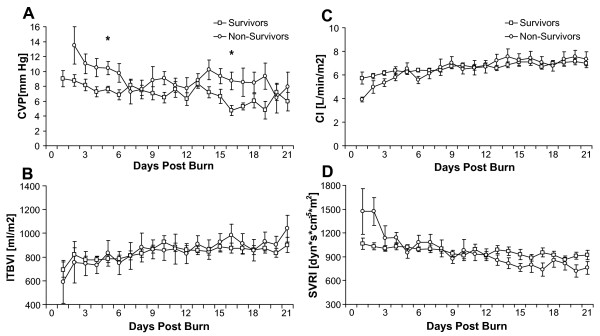
Seventy-nine patients with a mean age (±SD) of 9 ± 5 years and a mean TBSA burn (±SD) of 64% ± 20% were studied. CI significantly increased compared to level at admission and was highest 3 weeks postburn. ITBVI increased significantly starting at 8 days postburn. SVRI continuously decreased early in the perioperative burn period. EVLWI increased significantly starting at 9 days postburn. Young children (0 to 5 years old) had a significantly increased EVLWI and decreased ITBVI compared to older children (12 to 18 years old). EVLWI was significantly higher in patients who did not survive burn injury.
Continuous PiCCO measurements were performed for the first time in a large cohort of severely burned pediatric patients. The results suggest that hyperdynamic circulation begins within the first week after burn injury and continues throughout the entire intensive care unit stay.
严重烧伤后监测血流动力学和容量参数至关重要。然而,肺动脉导管与许多风险相关。我们的目的是展示在严重烧伤的儿科患者中使用微创经肺热稀释(TPTD)进行连续监测的可行性。
这项前瞻性队列研究纳入了总体表烧伤面积(TBSA)超过 40%且在受伤后 96 小时内入院的严重烧伤患者。使用 PiCCO 系统(德国慕尼黑的 Pulsion Medical Systems)进行 TPTD 测量。记录心指数(CI)、胸腔内血容量指数(ITBVI)(Stewart-Hamilton 方程)、血管外肺水指数(EVLWI)和全身血管阻力指数(SVRI)测量值,每天测量两次。使用单向重复测量方差分析进行统计分析,并进行组内和组间比较的事后 Bonferroni 检验。
研究纳入了 79 名年龄(±标准差)为 9 ± 5 岁、TBSA 烧伤(±标准差)为 64% ± 20%的患者。与入院时相比,CI 显著增加,烧伤后 3 周时达到最高水平。从烧伤后第 8 天开始,ITBVI 显著增加。SVRI 在围手术期烧伤早期持续下降。从烧伤后第 9 天开始,EVLWI 显著增加。与年龄较大的儿童(12 至 18 岁)相比,年龄较小的儿童(0 至 5 岁)的 EVLWI 显著增加,ITBVI 显著降低。未存活烧伤损伤的患者的 EVLWI 显著升高。
首次在大量严重烧伤儿科患者中进行连续 PiCCO 测量。结果表明,高动力循环在烧伤损伤后第一周内开始,并持续整个重症监护病房住院期间。