Schachter Michael E, Romann Alexandra, Djurdev Ognjenka, Levin Adeera, Beaulieu Monica
British Columbia Provincial Renal Agency, 700, 1380 Burrard Street, Vancouver BC V6Z 2H3, Canada.
BMC Nephrol. 2013 Aug 29;14:182. doi: 10.1186/1471-2369-14-182.
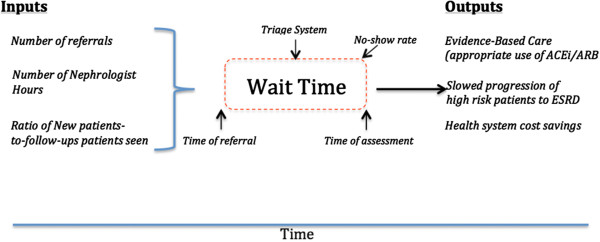
Early referral and management of high-risk chronic kidney disease may prevent or delay the need for dialysis. Automatic eGFR reporting has increased demand for out-patient nephrology consultations and in some cases, prolonged queues. In Canada, a national task force suggested the development of waiting time targets, which has not been done for nephrology.
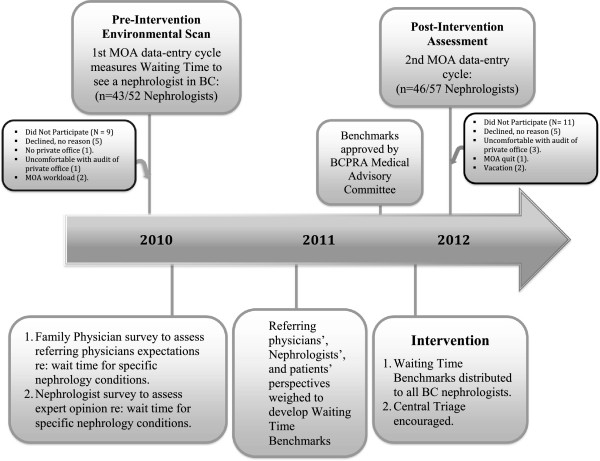
We sought to describe waiting time for outpatient nephrology consultations in British Columbia (BC). Data collection occurred in 2 phases: 1) Baseline Description (Jan 18-28, 2010) and 2) Post Waiting Time Benchmark-Introduction (Jan 16-27, 2012). Waiting time was defined as the interval from receipt of referral letters to assessment. Using a modified Delphi process, Nephrologists and Family Physicians (FP) developed waiting time targets for commonly referred conditions through meetings and surveys. Rules were developed to weigh-in nephrologists', FPs', and patients' perspectives in order to generate waiting time benchmarks. Targets consider comorbidities, eGFR, BP and albuminuria. Referred conditions were assigned a priority score between 1-4. BC nephrologists were encouraged to centrally triage referrals to see the first available nephrologist. Waiting time benchmarks were simultaneously introduced to guide patient scheduling. A post-intervention waiting time evaluation was then repeated.
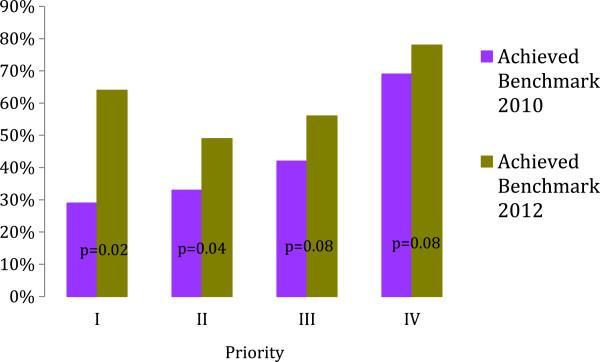
In 2010 and 2012, 43/52 (83%) and 46/57 (81%) of BC nephrologists participated. Waiting time decreased from 98(IQR44,157) to 64(IQR21,120) days from 2010 to 2012 (p = <.001), despite no change in referral eGFR, demographics, nor number of office hrs/wk. Waiting time improved most for high priority patients.
An integrated, Provincial initiative to measure wait times, develop waiting benchmarks, and engage physicians in active waiting time management associated with improved access to nephrologists in BC. Improvements in waiting time was most marked for the highest priority patients, which suggests that benchmarks had an influence on triaging behavior. Further research is needed to determine whether this effect is sustainable.
高危慢性肾脏病的早期转诊和管理可能预防或延迟透析需求。自动估算肾小球滤过率(eGFR)报告增加了门诊肾内科会诊需求,在某些情况下还导致候诊队伍延长。在加拿大,一个全国性特别工作组建议制定候诊时间目标,但肾内科尚未这样做。
我们试图描述不列颠哥伦比亚省(BC省)门诊肾内科会诊的候诊时间。数据收集分两个阶段进行:1)基线描述(2010年1月18日至28日)和2)引入候诊时间基准后(2012年1月16日至27日)。候诊时间定义为从收到转诊信到进行评估的间隔时间。通过改良的德尔菲法,肾内科医生和家庭医生(FP)通过会议和调查为常见转诊病情制定了候诊时间目标。制定了规则以权衡肾内科医生、家庭医生和患者的观点,从而生成候诊时间基准。目标考虑了合并症、eGFR、血压和蛋白尿。将转诊病情分配1至4之间的优先分数。鼓励BC省的肾内科医生集中对转诊进行分诊,以便由首位有空的肾内科医生诊治。同时引入候诊时间基准以指导患者安排。然后重复进行干预后候诊时间评估。
2010年和2012年,BC省分别有43/52(83%)和46/57(81%)的肾内科医生参与。从2010年到2012年,候诊时间从98(四分位间距44,157)天降至64(四分位间距21,120)天(p = <.001),尽管转诊的eGFR、人口统计学特征以及每周门诊小时数均无变化。高优先级患者的候诊时间改善最为明显。
一项省级综合举措,用于测量候诊时间、制定候诊基准,并让医生积极参与候诊时间管理,这与BC省改善肾内科医生的可及性相关。最高优先级患者的候诊时间改善最为显著,这表明基准对分诊行为产生了影响。需要进一步研究以确定这种效果是否可持续。