Harvard Medical School, Boston, MA, USA,
Dig Dis Sci. 2014 Jan;59(1):174-82. doi: 10.1007/s10620-013-2832-5. Epub 2013 Aug 30.
Hospital admissions in cirrhotic patients are a source of significant health care expenditure. Most studies to date have focused on readmissions in patients with decompensated cirrhosis. We sought to describe predictors of hospital admissions in an ambulatory cirrhosis cohort consisting of both compensated and decompensated patients to identify patients who could benefit from intensified outpatient chronic disease management.
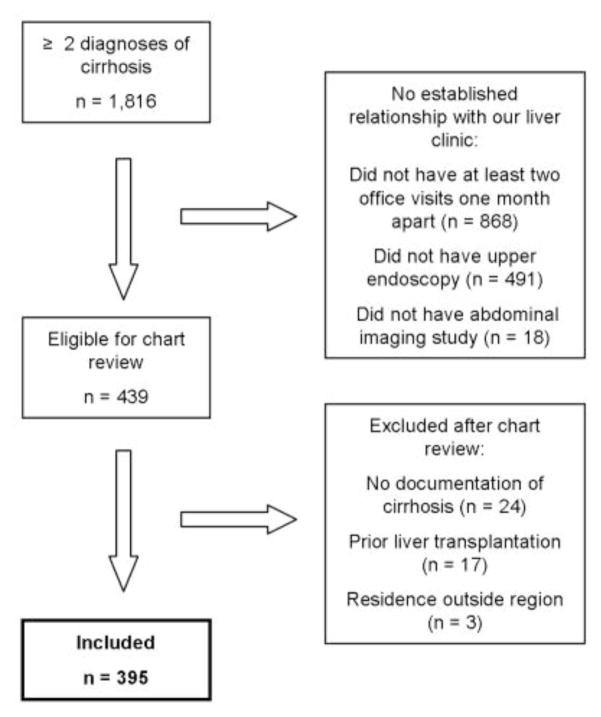
We performed a retrospective cohort study of 395 cirrhotic patients followed at an academic medical center liver clinic. Inclusion criteria were documented cirrhosis and longitudinal care at our center during 2006-2008. Patients were followed until December 2011, death, or liver transplantation. The primary outcomes were non-elective cirrhosis-related hospital admissions within 1 year and time to admission. The secondary outcome was 2-year cirrhosis-related mortality. The study was approved by the Partners Human Research Committee (protocol 2012P001912).
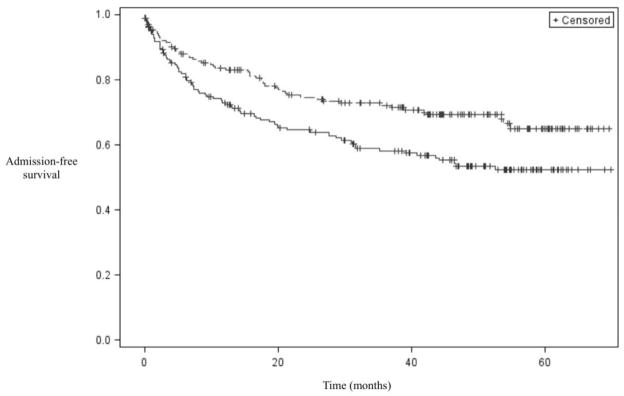
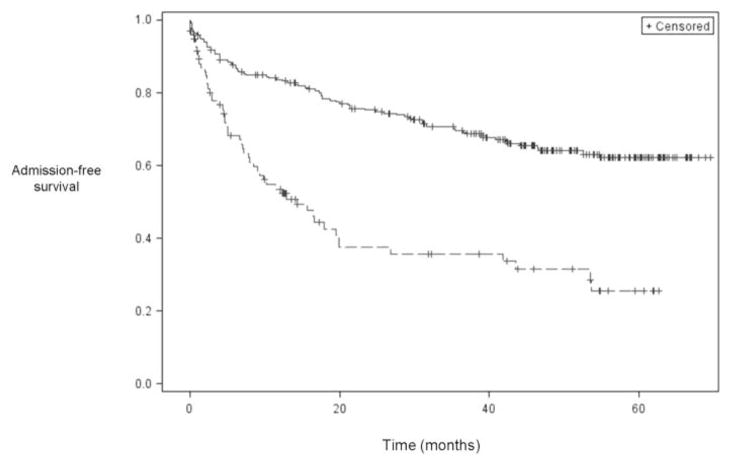
Seventy-eight patients (19.7 %) had at least one cirrhosis-related hospital admission within 1 year. The following were significant predictors in the multivariable model: model for end-stage liver disease score ≥15 [OR 2.22, 95 % CI (1.21-4.07), p = 0.01], diagnosis of hepatocellular carcinoma [3.64 (1.42-9.35), 0.007], diuretic use [2.27 (1.23-4.17), 0.008], at least one cirrhosis-related admission during the baseline year [2.17 (1.21-3.89), 0.01], and being unmarried [1.92 (1.10-3.35), 0.02].
Advanced disease, diuretic use, and marital status were associated with cirrhosis-related hospital admissions in patients followed at an academic medical center liver clinic. Our findings suggest that patients with inadequately or overzealously treated ascites, as well as those with limited social supports, could benefit from intensified outpatient management.
肝硬化患者的住院治疗是医疗保健支出的主要来源。迄今为止,大多数研究都集中在失代偿性肝硬化患者的再入院上。我们旨在描述一个由代偿和失代偿性肝硬化患者组成的门诊肝硬化队列的住院预测因素,以确定那些可能受益于强化门诊慢性病管理的患者。
我们对在学术医疗中心肝脏诊所接受治疗的 395 例肝硬化患者进行了回顾性队列研究。纳入标准为 2006 年至 2008 年期间在我院确诊的肝硬化患者,并接受了长期治疗。患者随访至 2011 年 12 月,死亡或进行肝移植。主要转归为 1 年内非择期肝硬化相关的住院治疗和入院时间。次要结局为 2 年肝硬化相关死亡率。该研究得到了合作伙伴人类研究委员会(方案号 2012P001912)的批准。
78 例患者(19.7%)在 1 年内至少有 1 次肝硬化相关住院治疗。多变量模型中的显著预测因素包括:终末期肝病模型评分≥15 [比值比(OR)2.22,95%置信区间(CI)1.21-4.07),p = 0.01]、肝细胞癌诊断(OR 3.64,95%CI 1.42-9.35),0.007]、利尿剂使用(OR 2.27,95%CI 1.23-4.17),0.008]、基线年内至少有 1 次肝硬化相关入院[OR 2.17,95%CI 1.21-3.89),0.01]和未婚[OR 1.92,95%CI 1.10-3.35),0.02]。
在学术医疗中心肝脏诊所接受治疗的患者中,晚期疾病、利尿剂使用和婚姻状况与肝硬化相关的住院治疗有关。我们的研究结果表明,那些腹水治疗不足或过度的患者,以及那些社会支持有限的患者,可能受益于强化门诊管理。