Department of Medical Imaging, Jinling Hospital, Medical School of Nanjing University, Nanjing, China ; School of Medical Imaging, Xuzhou Medical College, Xuzhou, China.
PLoS One. 2013 Aug 22;8(8):e71507. doi: 10.1371/journal.pone.0071507. eCollection 2013.
To investigate the pattern of spontaneous neural activity in patients with end-stage renal disease (ESRD) with and without neurocognitive dysfunction using resting-state functional magnetic resonance imaging (rs-fMRI) with a regional homogeneity (ReHo) algorithm.
rs-fMRI data were acquired in 36 ESRD patients (minimal nephro-encephalopathy [MNE], n = 19, 13 male, 37±12.07 years; non-nephro-encephalopathy [non-NE], n = 17, 11 male, 38±12.13 years) and 20 healthy controls (13 male, 7 female, 36±10.27 years). Neuropsychological (number connection test type A [NCT-A], digit symbol test [DST]) and laboratory tests were performed in all patients. The Kendall's coefficient of concordance (KCC) was used to measure the regional homogeneity for each subject. The regional homogeneity maps were compared using ANOVA tests among MNE, non-NE, and healthy control groups and post hoc t -tests between each pair in a voxel-wise way. A multiple regression analysis was performed to evaluate the relationships between ReHo index and NCT-A, DST scores, serum creatinine and urea levels, disease and dialysis duration.
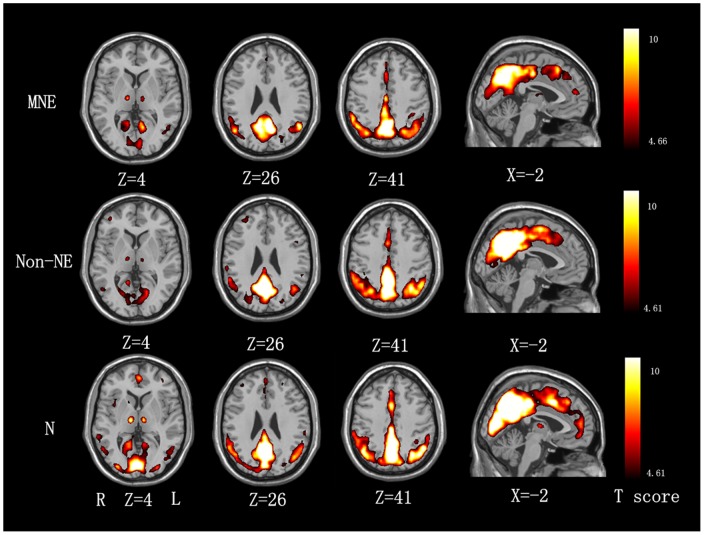
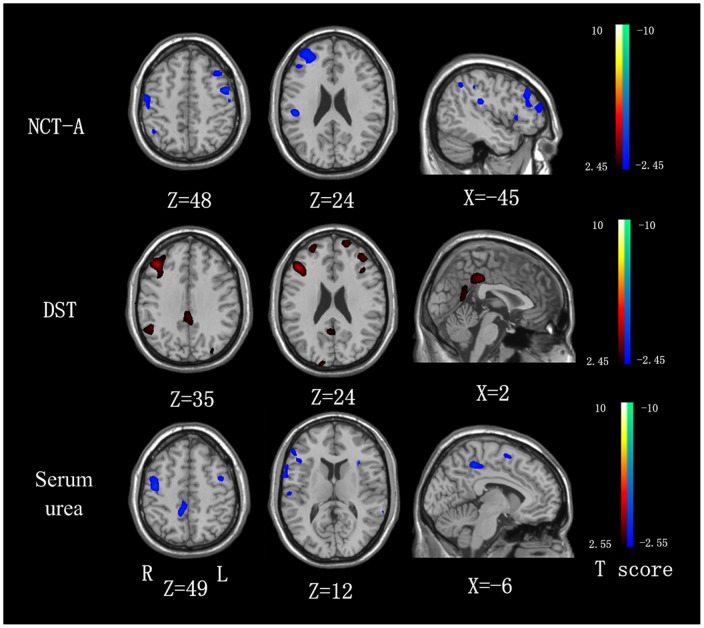
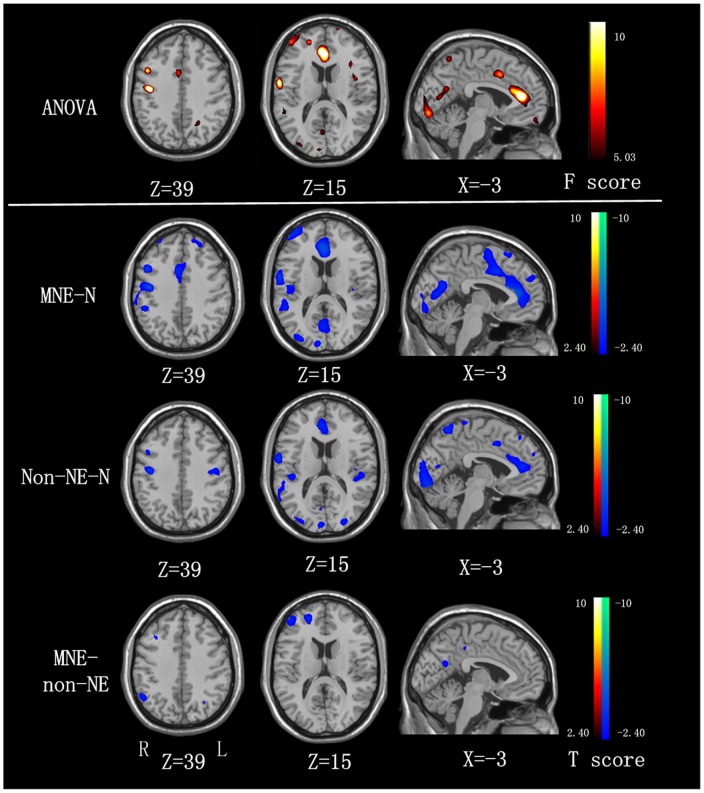
Compared with healthy controls, both MNE and non-NE patients showed decreased ReHo in the multiple areas of bilateral frontal, parietal and temporal lobes. Compared with the non-NE, MNE patients showed decreased ReHo in the right inferior parietal lobe (IPL), medial frontal cortex (MFC) and left precuneus (PCu). The NCT-A scores and serum urea levels of ESRD patients negatively correlated with ReHo values in the frontal and parietal lobes, while DST scores positively correlated with ReHo values in the bilateral PCC/precuneus, MFC and inferior parietal lobe (IPL) (all P<0.05, AlphaSim corrected). No significant correlations were found between any regional ReHo values and disease duration, dialysis duration and serum creatinine values in ESRD patients (all P>0.05, AlphaSim corrected).
Diffused decreased ReHo values were found in both MNE and non-NE patients. The progressively decreased ReHo in the default mode network (DMN), frontal and parietal lobes might be trait-related in MNE. The ReHo analysis may be potentially valuable for elucidating neurocognitive abnormalities of ESRD patients and detecting the development from non-NE to MNE.
使用局部一致性(ReHo)算法的静息态功能磁共振成像(rs-fMRI)研究终末期肾病(ESRD)患者有无神经认知功能障碍的自发性神经活动模式。
共纳入 36 例 ESRD 患者(最小肾脑病[MNE],n = 19,男 13 例,年龄 37±12.07 岁;非肾脑病[non-NE],n = 17,男 11 例,年龄 38±12.13 岁)和 20 名健康对照者(男 13 名,女 7 名,年龄 36±10.27 岁)进行 rs-fMRI 检查。所有患者均行神经心理学检查(数字连接测试 A[NCT-A],数字符号测试[DST])和实验室检查。Kendall 一致性系数(KCC)用于测量每个受试者的局部一致性。采用方差分析比较 MNE、non-NE 和健康对照组之间的局部一致性图,然后在体素水平上进行两两比较的 t 检验。采用多元回归分析评估 ReHo 指数与 NCT-A、DST 评分、血清肌酐和尿素水平、疾病和透析时间的关系。
与健康对照组相比,MNE 和 non-NE 患者双侧额、顶、颞叶多个区域的 ReHo 均降低。与 non-NE 相比,MNE 患者右侧顶下小叶(IPL)、内侧额皮质(MFC)和左侧楔前叶(PCu)的 ReHo 降低。ESRD 患者的 NCT-A 评分和血清尿素水平与额叶和顶叶的 ReHo 值呈负相关,而 DST 评分与双侧后扣带回/楔前叶(PCC/precuneus)、MFC 和 IPL 的 ReHo 值呈正相关(均 P<0.05,AlphaSim 校正)。ESRD 患者任何区域的 ReHo 值与疾病持续时间、透析时间和血清肌酐值均无显著相关性(均 P>0.05,AlphaSim 校正)。
MNE 和 non-NE 患者均存在弥漫性 ReHo 值降低。DMN、额叶和顶叶默认模式网络(DMN)的 ReHo 值逐渐降低可能与 MNE 的特征有关。ReHo 分析可能有助于阐明 ESRD 患者的神经认知异常,并检测从 non-NE 到 MNE 的发展。