Department of Diabetology, Endocrinology and Nutrition, CHU Hospital Grenoble, and University Joseph Fourier, Grenoble, France.
Diabetes Ther. 2013 Dec;4(2):385-98. doi: 10.1007/s13300-013-0038-7. Epub 2013 Aug 31.
To assess in real life the rate of hypoglycemia during Ramadan in patients with type 2 diabetes (T2DM) in France, according to their ongoing dual therapy of metformin-vildagliptin or metformin-sulfonylurea/glinide (IS).
Prospective, non-interventional study with 2 visits (within 8 weeks before and 6 weeks after the end of Ramadan 2012). Study diaries were not used to collect events or record values of glucose monitoring. One hundred and ninety-eight patients on stable oral dual therapy for ≥2 months and with glycosylated hemoglobin (HbA1c) ≤8.0% were recruited by 62 centers: 83 in the IS cohort and 115 in the vildagliptin cohort.
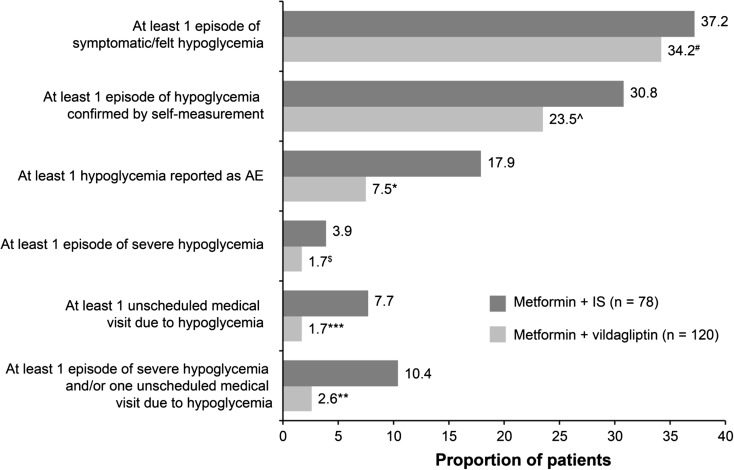
Approximately 90% of patients were from Maghreb. The two cohorts were well balanced: 60% men, mean age 59 years, BMI 28 kg/m(2), metformin dose ~2,000 mg/day, and HbA1c 7.2%. Distinct therapeutic management was planned in view of Ramadan with drug-adaptation intended in 61.4% of IS and 18.3% of vildagliptin patients. Hypoglycemia was reported in 37% of IS and 34% of vildagliptin patients; episodes declared as confirmed in 30.8% and 23.5%, respectively, and episodes documented as adverse event (AE) in 17.9% (22 episodes) and 7.5% (13 episodes), respectively (P = 0.025). Severe episodes were reported in 3.9% of IS and 1.7% of vildagliptin patients. 10.4% of IS and 2.6% of vildagliptin patients reported severe episodes and/or unscheduled medical visits due to hypoglycemia (P = 0.029). Glycemic control remained stable in both cohorts. Compliance with fasting was high, as well as adherence to drug with ≥5 missed-dose for 15.4% of IS and 8.5% of vildagliptin patients.
Although the overall frequency of malaise suggestive of hypoglycemia was high, which would be expected with prolonged fasting in a well-controlled T2DM population during hot summer days, the incidence of more severe and better-documented episodes (AE, severe event, event leading to unscheduled medical visit) were much lower, with consistently less events with vildagliptin therapy.
在法国,根据正在进行的二甲双胍-维格列汀或二甲双胍-磺酰脲/格列奈双联治疗,评估 2 型糖尿病(T2DM)患者在斋月期间的低血糖发生率。
前瞻性、非干预性研究,共进行 2 次访视(在 2012 年斋月结束前 8 周内和结束后 6 周内)。研究日记未用于收集事件或记录血糖监测值。通过 62 个中心招募了 198 名稳定接受双联口服治疗≥2 个月且糖化血红蛋白(HbA1c)≤8.0%的患者:83 名患者来自 IS 队列,115 名患者来自维格列汀队列。
约 90%的患者来自马格里布地区。两个队列之间平衡良好:60%为男性,平均年龄 59 岁,BMI 28kg/m2,二甲双胍剂量约 2000mg/天,HbA1c 7.2%。鉴于斋月,计划了不同的治疗管理,IS 组中 61.4%和维格列汀组中 18.3%的患者计划调整药物。IS 组和维格列汀组分别有 37%和 34%的患者报告低血糖;分别有 30.8%和 23.5%的患者报告确认的发作,17.9%(22 例)和 7.5%(13 例)的发作记录为不良事件(AE),分别(P=0.025)。IS 组和维格列汀组分别有 3.9%和 1.7%的患者报告严重发作。IS 组和维格列汀组分别有 10.4%和 2.6%的患者报告因低血糖而出现严重发作和/或计划外就诊(P=0.029)。两个队列的血糖控制均保持稳定。禁食的依从性很高,IS 组和维格列汀组分别有 15.4%和 8.5%的患者至少漏服 1 剂药物 5 次以上。
尽管在炎热的夏日里,在血糖控制良好的 T2DM 人群中长时间禁食,导致低血糖相关不适症状的总体发生率较高,但更严重和记录更完善的发作(AE、严重事件、导致计划外就诊的事件)发生率较低,维格列汀治疗的发作事件更少。