Molina Luis, Sutton Richard, Gandoy William, Reyes Nicolás, Lara Susano, Limón Froylán, Gómez Susana, Orihuela Consuelo, Salame Latife, Moreno Gabriela
Arrhythmia Laboratory of the Universidad Nacional Autónoma de México (UNAM) en Hospital General de México, Mexico City, Medico.
Pacing Clin Electrophysiol. 2014 Feb;37(2):207-14. doi: 10.1111/pace.12257. Epub 2013 Sep 2.
Pacing the right ventricle is established practice, but there remains controversy as to the optimal site to preserve hemodynamic function.
To evaluate clinical and hemodynamic differences between apical and septal pacing in pacemaker-dependent patients.
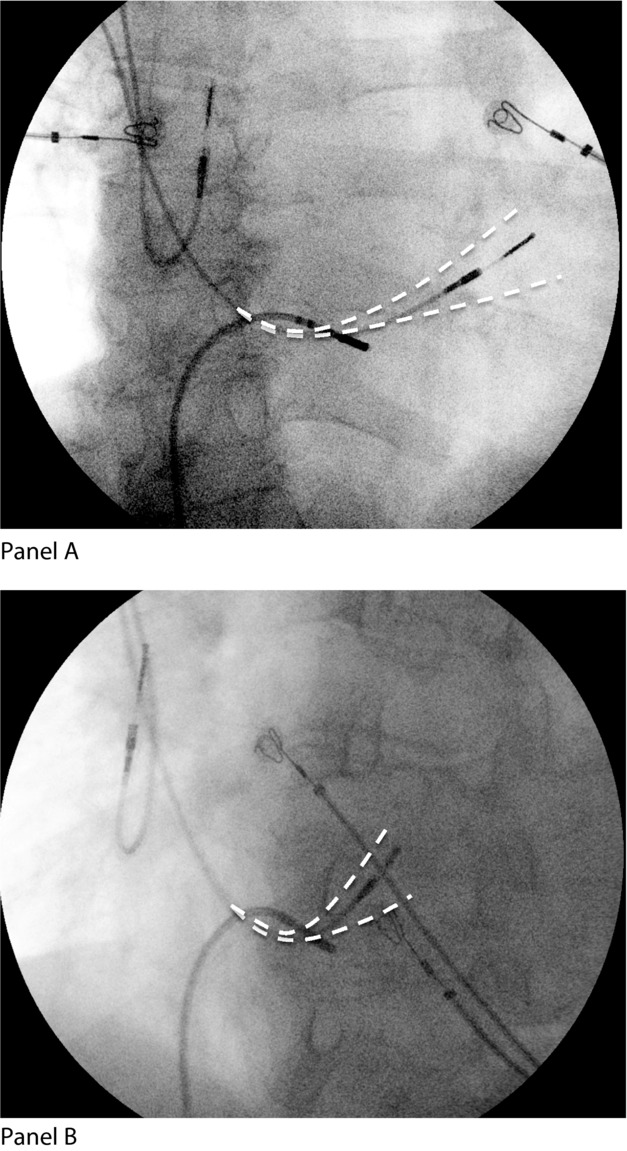
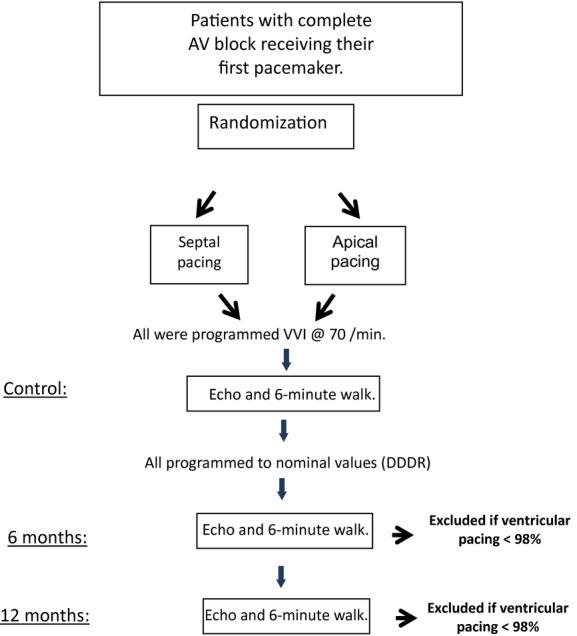
Patients receiving their first pacemaker for advanced atrioventricular block, with the atria in sinus rhythm, were randomized to receive apical (Group A) or septal (Group S) ventricular leads. After implant, with the device programmed VVI 70 beats/min fixed rate, patients underwent a 6-minute walk test and a transthoracic echocardiogram. Then, DDDR was programmed at nominal settings. The same tests were performed at 6 months and 12 months follow-up. If ventricular pacing was less than 98%, the patient was excluded.
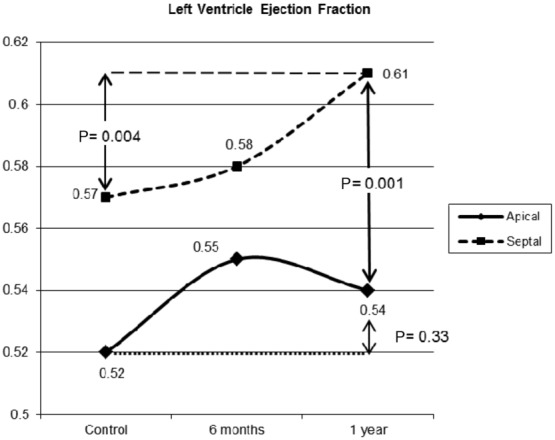
A total of 142 patients were included in the study. During the study year, 71 (50%) were excluded for not fulfilling the condition of 98% ventricular pacing. Groups A and S had 34 and 37 patients, respectively. Age and gender were similar in the groups. At implant, QRS duration was significantly greater in Group A (158 ms) than Group S (146 ms; P = 0.018), and the QRS axis was different: -74.5° in Group A and 1° in Group S (P < 0.001). At 1 year, the 6-minute walk improved significantly in both groups: Group A 15% (P = 0.048) and Group S 24% (P = 0.001). Left ventricular ejection fraction (LVEF) increased from 0.57 to 0.61 (P = 0.008) in Group S, without significant change in Group A.
After 1 year, pacemaker-dependent patients with septal ventricular leads have better clinical and functional (LVEF) outcome.
右心室起搏是既定的做法,但对于保留血流动力学功能的最佳部位仍存在争议。
评估起搏器依赖患者心尖部起搏和间隔部起搏之间的临床及血流动力学差异。
因高度房室传导阻滞首次接受起搏器治疗且心房为窦性心律的患者,被随机分为接受心尖部(A组)或间隔部(S组)心室电极植入。植入后,将设备程控为VVI 70次/分钟固定频率,患者接受6分钟步行试验和经胸超声心动图检查。然后,将DDDR程控为标称设置。在6个月和12个月随访时进行相同检查。如果心室起搏比例低于98%,则将患者排除。
共有142例患者纳入研究。在研究年度内,71例(50%)因未达到98%心室起搏条件而被排除。A组和S组分别有34例和37例患者。两组患者年龄和性别相似。植入时,A组QRS时限(158毫秒)显著长于S组(146毫秒;P = 0.018),且QRS电轴不同:A组为-74.5°,S组为1°(P < 0.001)。1年时,两组6分钟步行距离均显著改善:A组改善15%(P = 0.048),S组改善24%(P = 0.001)。S组左心室射血分数(LVEF)从0.57升至0.61(P = 0.008),A组无显著变化。
1年后,植入间隔部心室电极的起搏器依赖患者有更好的临床和功能(LVEF)结局。