Transplants, Cell therapy and Regenerative Medicine Unit, Hospital Universitario Central de Asturias, Oviedo, Spain.
PLoS One. 2013 Aug 29;8(8):e73526. doi: 10.1371/journal.pone.0073526. eCollection 2013.
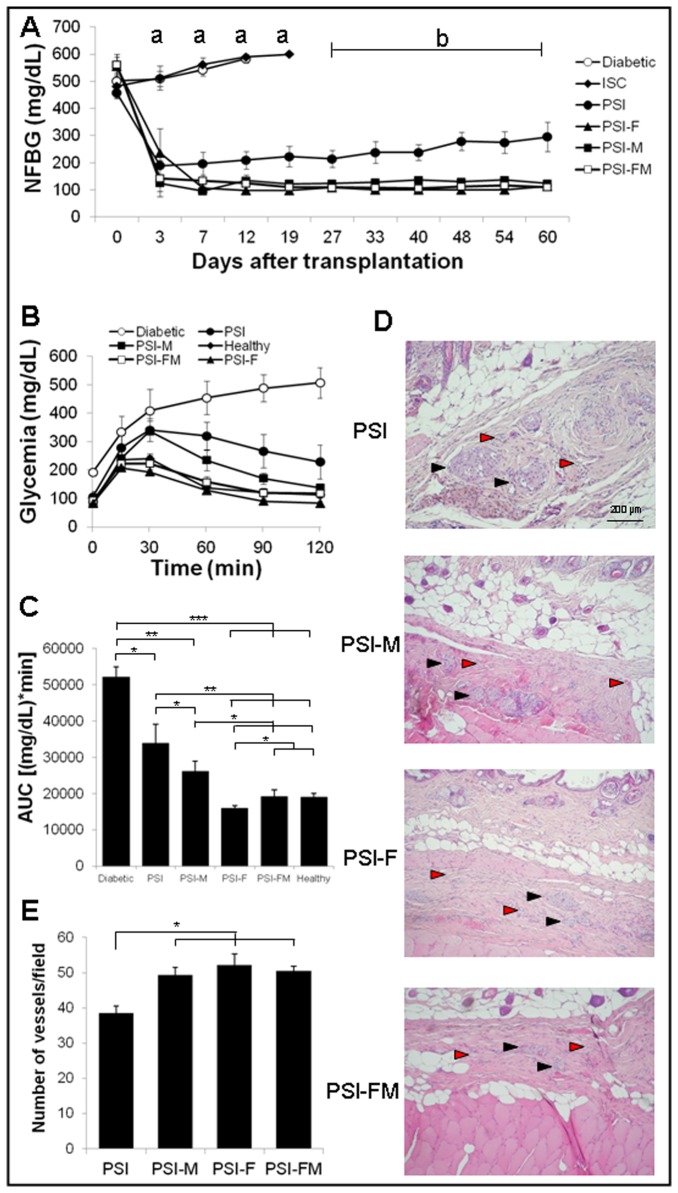
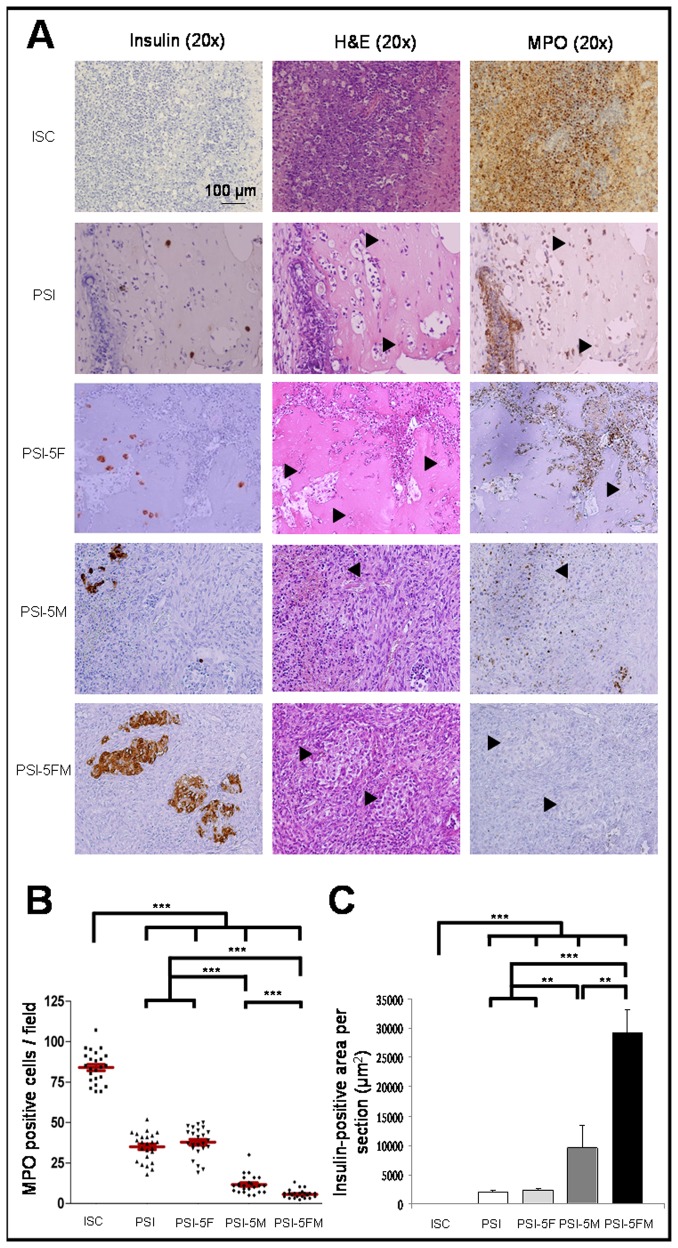
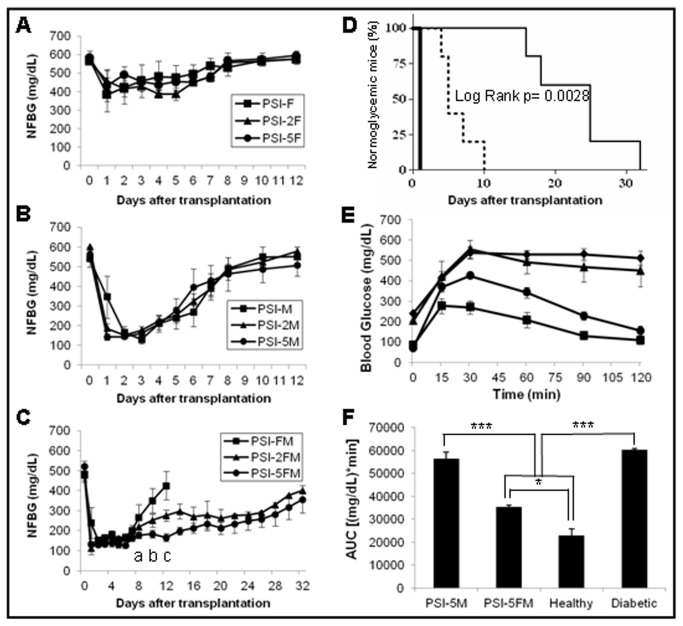
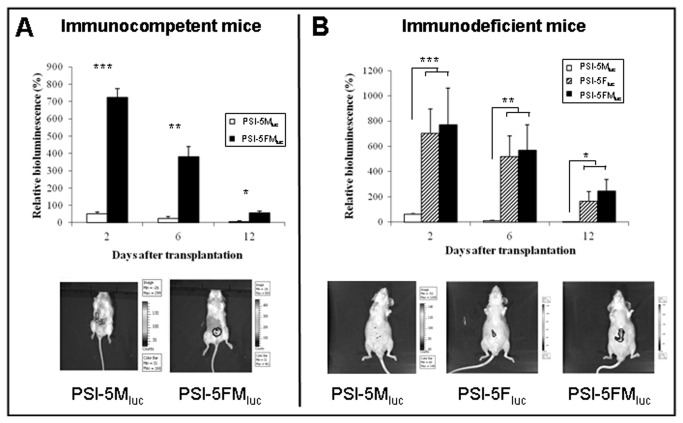
Experimental and clinical experiences highlight the need to review some aspects of islet transplantation, especially with regard to site of grafting and control of the immune response. The subcutaneous space could be a good alternative to liver but its sparse vasculature is its main limitation. Induction of graft tolerance by using cells with immunoregulatory properties is a promising approach to avoid graft rejection. Both Fibroblasts and Mesenchymal Stem Cells (MSCs) have shown pro-angiogenic and immunomodulatory properties. Transplantation of islets into the subcutaneous space using plasma as scaffold and supplemented with fibroblasts and/or Bone Marrow-MSCs could be a promising strategy to achieve a functional extra-hepatic islet graft, without using immunosuppressive drugs. Xenogenic rat islets, autologous fibroblasts and/or allogenic BM-MSCs, were mixed with plasma, and coagulation was induced to constitute a Plasma-based Scaffold containing Islets (PSI), which was transplanted subcutaneously both in immunodeficient and immunocompetent diabetic mice. In immunodeficient diabetic mice, PSI itself allowed hyperglycemia reversion temporarily, but the presence of pro-angiogenic cells (fibroblasts or BM-MSCs) within PSI was necessary to improve graft re-vascularization and, thus, consistently maintain normoglycemia. In immunocompetent diabetic mice, only PSI containing BM-MSCs, but not those containing fibroblasts, normalized glycemia lasting up to one week after transplantation. Interestingly, when PSI contained both fibroblasts and BM-MSCs, the normoglycemia period showed an increase of 4-times with a physiological-like response in functional tests. Histology of immunocompetent mice showed an attenuation of the immune response in those grafts with BM-MSCs, which was improved by co-transplantation with fibroblasts, since they increased BM-MSC survival. In summary, fibroblasts and BM-MSCs showed similar pro-angiogenic properties in this model of islet xenotransplantation, whereas only BM-MSCs exerted an immunomodulatory effect, which was improved by the presence of fibroblasts. These results suggest that cooperation of different cell types with islets will be required to achieve a long-term functional graft.
实验和临床经验强调需要重新审视胰岛移植的一些方面,特别是关于移植物部位和免疫反应控制的问题。皮下空间可能是肝脏的一个很好的替代选择,但它稀疏的脉管系统是其主要限制。使用具有免疫调节特性的细胞诱导移植物耐受是避免移植物排斥的一种很有前途的方法。成纤维细胞和间充质干细胞 (MSCs) 都具有促血管生成和免疫调节特性。使用纤维母细胞和/或骨髓间充质干细胞作为支架将胰岛移植到皮下空间,并补充纤维母细胞和/或骨髓间充质干细胞,可能是实现无免疫抑制药物的功能性肝外胰岛移植物的一种很有前途的策略。将异种大鼠胰岛、自体成纤维细胞和/或同种异体 BM-MSCs 与血浆混合,诱导凝固形成含有胰岛的血浆基支架(PSI),将其移植到免疫缺陷和免疫活性糖尿病小鼠的皮下。在免疫缺陷糖尿病小鼠中,PSI 本身可以暂时逆转高血糖,但 PSI 内存在促血管生成细胞(成纤维细胞或 BM-MSCs)是改善移植物再血管化所必需的,从而持续维持正常血糖。在免疫活性糖尿病小鼠中,只有含有 BM-MSCs 的 PSI 而不是含有成纤维细胞的 PSI 能使血糖正常化,持续时间长达移植后一周。有趣的是,当 PSI 同时含有成纤维细胞和 BM-MSCs 时,正常血糖期增加了 4 倍,并且在功能测试中表现出类似生理的反应。免疫活性小鼠的组织学显示,在含有 BM-MSCs 的移植物中,免疫反应减弱,而与成纤维细胞共移植可改善这种情况,因为成纤维细胞增加了 BM-MSC 的存活率。总之,在胰岛异种移植的这种模型中,成纤维细胞和 BM-MSCs 表现出相似的促血管生成特性,而只有 BM-MSCs 发挥免疫调节作用,与成纤维细胞的存在一起可改善这种作用。这些结果表明,需要不同类型的细胞与胰岛的合作才能实现长期功能移植物。