Division of Pulmonary, Critical Care, and Sleep Medicine, University of Cincinnati School of Medicine, Cincinnati, Ohio, USA ; Division of Pulmonary, Critical Care, and Sleep Medicine, University of Cincinnati School of Medicine, Cincinnati, Ohio, USA ; Division of Pulmonary, Allergy, Critical Care and Sleep Medicine, Davis Heart and Lung Research Institute, The Ohio State University, Columbus, Ohio, USA.
Pulm Circ. 2013 Apr;3(2):389-95. doi: 10.4103/2045-8932.113184.
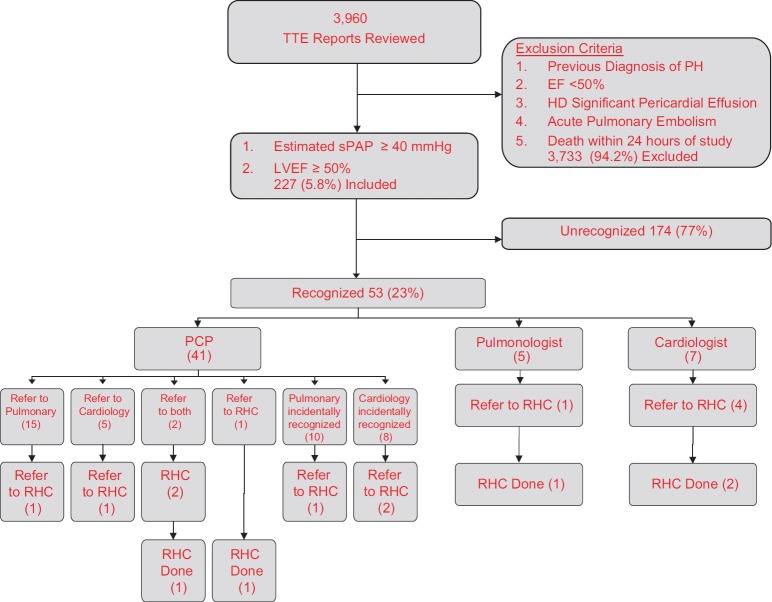
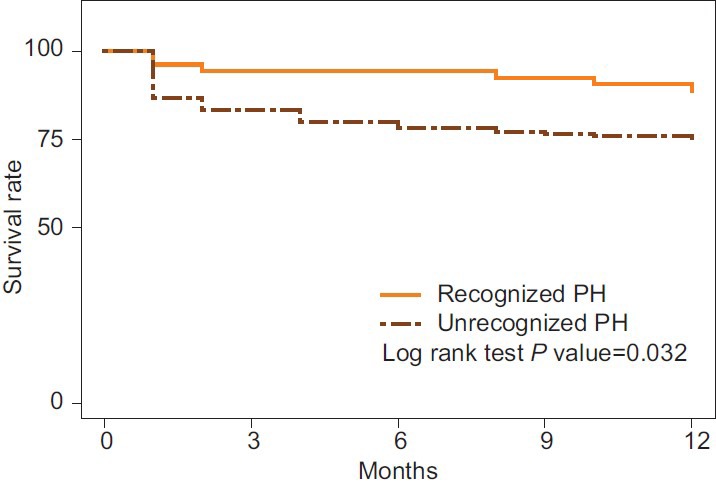
PH occurs alone or in association with many disorders. Many patients with transthoracic echocardiography (TTE) findings suggesting PH never receive additional evaluation. Patient characteristics and echocardiographic data associated with increased recognition of PH have not been fully evaluated. We evaluated TTE reports at the Cincinnati Veterans Affairs Medical Center from 2005 to 2006 retrospectively for findings highly indicative of PH: Estimated systolic pulmonary artery pressure (sPAP) ≥40 mmHg, increased right atrial or right ventricular (RV) size, or reduced RV function. Only patients with left ventricular ejection fraction (LVEF) ≥50% and no known diagnosis of PH were included. Patient characteristics, TTE findings, provider recognition rates, and subsequent referral for additional evaluation were assessed. A total of 227 of 3,960 (5.7%) TTE reports revealed findings indicating possible PH. Providers acknowledged possible PH in 53 (23.4%) reports. Recognized PH was predicted by increased RV size (odds ratio (OR) = 5.07, P < 0.001), increased right atrial dimension (OR = 6.45, P < 0.001), decreased RV function (OR = 8.86, P < 0.001), and increased PAP (OR = 1.04 corresponding to each unit increase of PAP, P < 0.01). Patients with comorbid obstructive sleep apnea (OSA), interstitial lung disease, and dyspnea were also more likely to be recognized (OR = 3.63, P = 0.021; OR = 10.98, P = 0.004; OR = 2.39, P = 0.007, respectively). The 12-month mortality rate for recognized patients, 11.3% (7/53), was lower than for unrecognized patients, 25.3% (44/174; P = 0.03). Providers recognized less than one in four patients with echocardiographic evidence suggesting PH. Echocardiography reports revealing higher PAP and right heart dilation and dysfunction are associated with increased acknowledgement of possible PH.
PH 可单独发生或与许多疾病相关。许多经胸超声心动图(TTE)检查结果提示 PH 的患者从未接受过额外的评估。与 PH 识别率增加相关的患者特征和超声心动图数据尚未得到充分评估。我们回顾性地评估了 2005 年至 2006 年辛辛那提退伍军人事务医疗中心的 TTE 报告,以寻找高度提示 PH 的发现:估计收缩期肺动脉压(sPAP)≥40mmHg、右心房或右心室(RV)增大或 RV 功能降低。仅纳入左心室射血分数(LVEF)≥50%且无已知 PH 诊断的患者。评估了患者特征、TTE 结果、提供者识别率以及随后是否转介进行额外评估。在 3960 份 TTE 报告中,有 227 份(5.7%)报告显示可能存在 PH 的发现。在 53 份(23.4%)报告中,提供者承认可能存在 PH。RV 增大(比值比(OR)=5.07,P<0.001)、右心房内径增大(OR=6.45,P<0.001)、RV 功能降低(OR=8.86,P<0.001)和 PAP 增加(OR=1.04,对应 PAP 每增加一个单位,P<0.01)可预测识别出 PH。患有共病阻塞性睡眠呼吸暂停(OSA)、间质性肺病和呼吸困难的患者也更有可能被识别(OR=3.63,P=0.021;OR=10.98,P=0.004;OR=2.39,P=0.007)。被识别出的患者的 12 个月死亡率为 11.3%(7/53),低于未被识别出的患者的 25.3%(44/174;P=0.03)。提供者识别出的具有超声心动图提示 PH 证据的患者不足四分之一。揭示更高 PAP 和右心扩张和功能障碍的超声心动图报告与 PH 可能性的识别增加相关。