Institute of Biomedical Engineering, National Research Council, Padova, Italy.
PLoS One. 2013 Sep 3;8(9):e73154. doi: 10.1371/journal.pone.0073154. eCollection 2013.
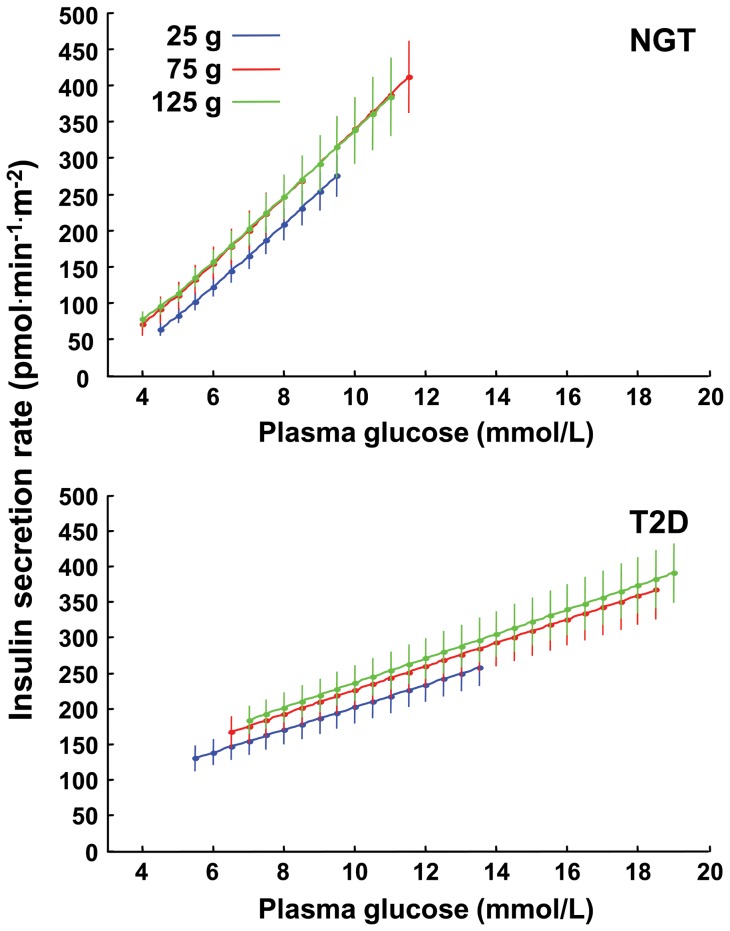
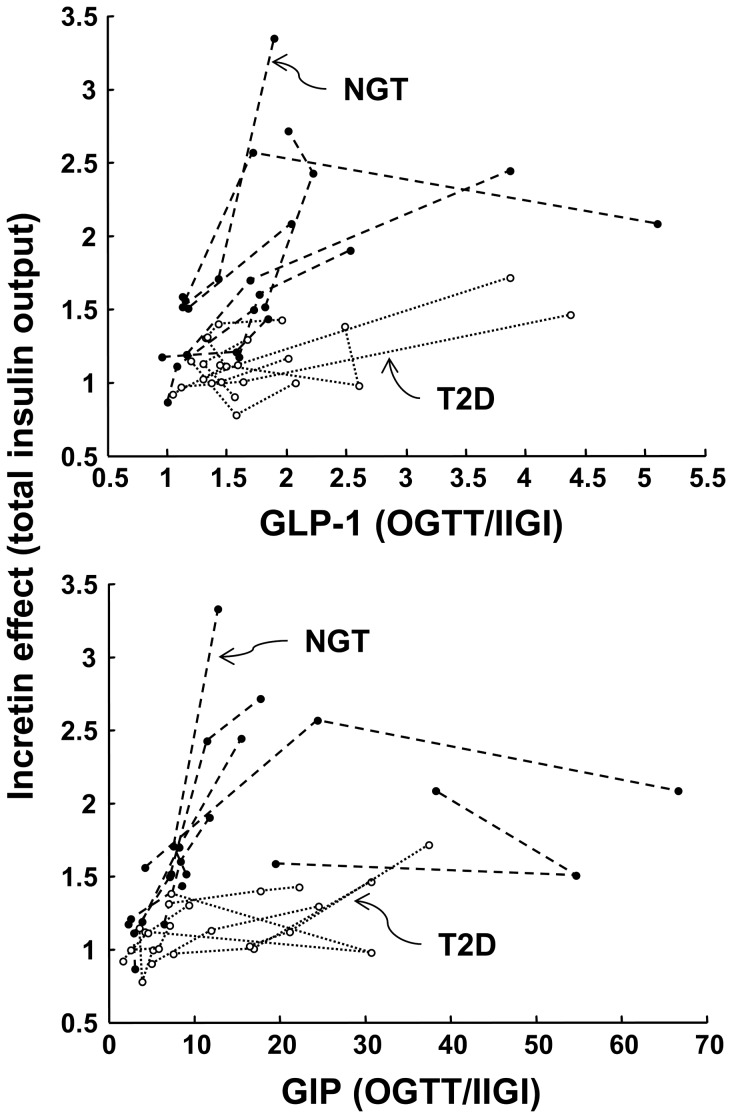
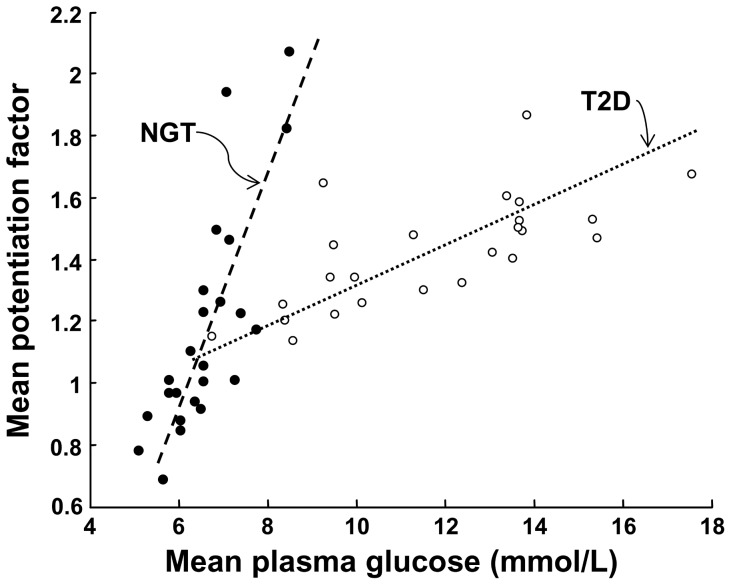
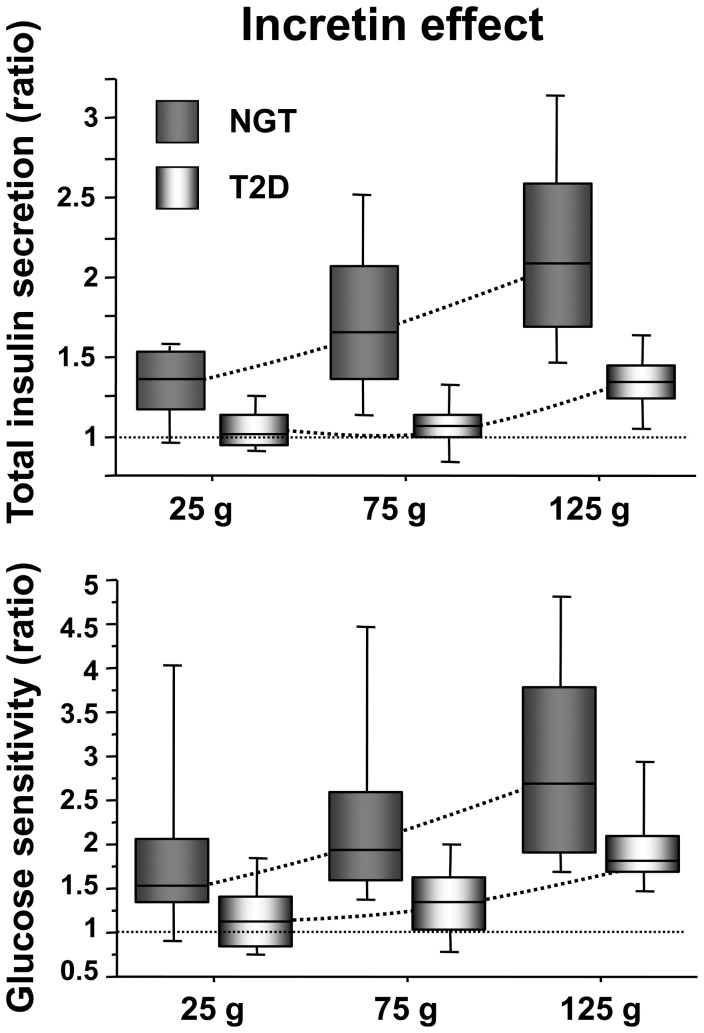
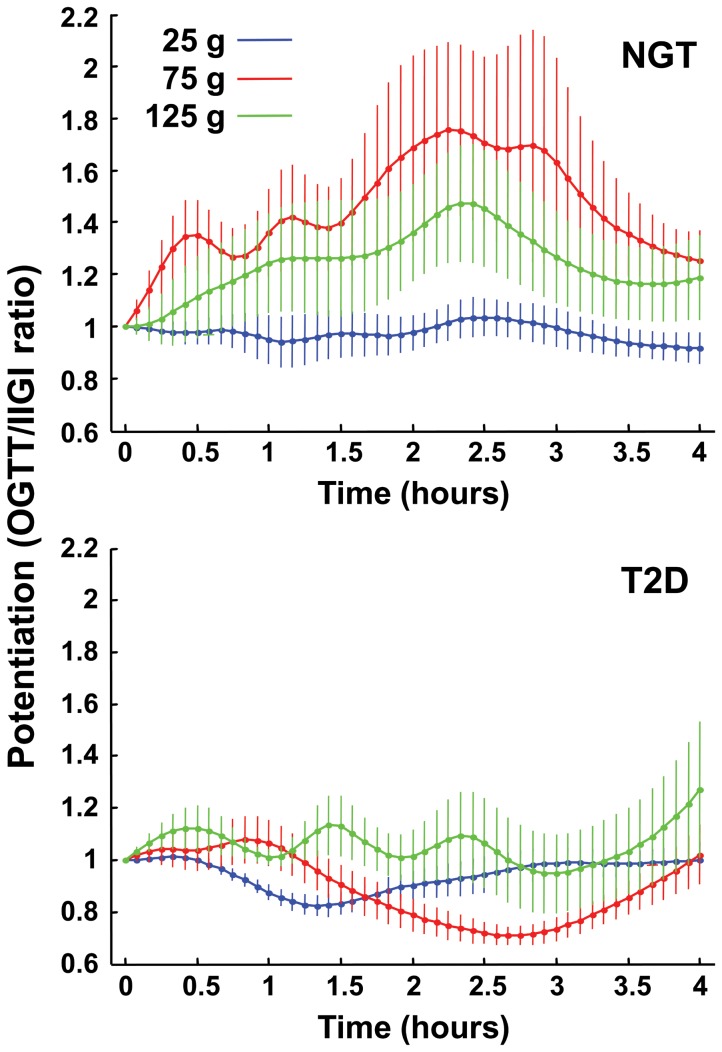
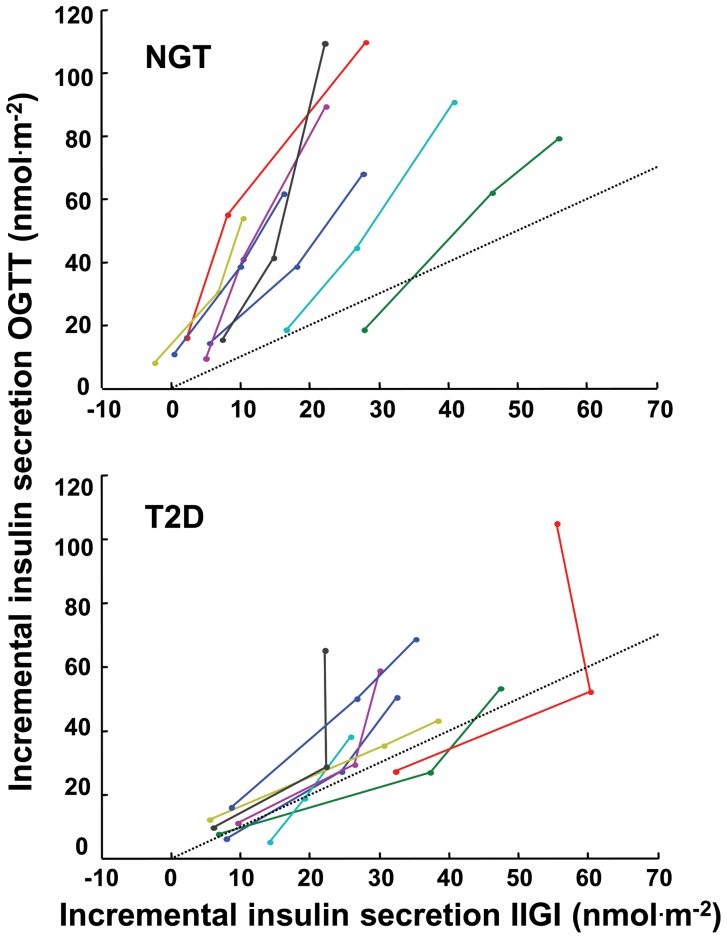
The incretin effect on insulin secretion was investigated in 8 subjects with type 2 diabetes (T2D) and 8 with normal glucose tolerance (NGT), using 25, 75, and 125 g oral glucose tolerance tests (OGTT) and isoglycemic intravenous glucose infusions (IIGI). The ß-cell response was evaluated using a model embedding a dose-response (slope=glucose sensitivity), an early response (rate sensitivity), and potentiation (time-related secretion increase). The incretin effect, as OGTT/IIGI ratio, was calculated for each parameter. In NGT, the incretin effect on total secretion increased with dose (1.3 ± 0.1, 1.7 ± 0.2, 2.2 ± 0.2 fold of IIGI, P<0.0001), mediated by a dose-dependent increase of the incretin effect on glucose sensitivity (1.9 ± 0.4, 2.4 ± 0.4, 3.1 ± 0.4, P=0.005), and a dose-independent enhancement of the incretin effect on rate sensitivity (894 [1145], 454 [516], 783 [1259] pmol m(-2) L mmol(-1) above IIGI; median [interquartile range], P<0.0001). The incretin effect on potentiation also increased (0.97 ± 0.06, 1.45 ± 0.20, 1.24 ± 0.16, P<0.0001). In T2D, the incretin effect on total secretion (1.0 ± 0.1, 1.1 ± 0.1, 1.3 ± 0.1, P=0.004) and glucose sensitivity (1.2 ± 0.2, 1.3 ± 0.2, 2.0 ± 0.2, P=0.005) were impaired vs NGT; however, the incretin effect on rate sensitivity increased already at 25 g (269 [169], 284 [301], 193 [465] pmol m(-2) L mmol(-1) above IIGI; negligible IIGI rate sensitivity in T2D prevented the calculation of the fold increment). OGTT did not stimulate potentiation above IIGI (0.94 ± 0.04, 0.89 ± 0.06, 1.06 ± 0.09; P<0.01 vs NGT). In the whole group, the incretin effect was inversely associated with total secretion during IIGI, although systematically lower in T2D. In conclusion, 1) In NGT, glucose sensitivity and potentiation mediate the dose-dependent incretin effect increase; 2) In T2D, the incretin effect is blunted vs NGT, but rate sensitivity is enhanced at all loads; 3) Relatively lower incretin effect in NGT is associated with higher secretion during IIGI, suggesting that the reduced incretin effect does not result from ß-cell dysfunction.
在 8 名 2 型糖尿病(T2D)患者和 8 名糖耐量正常(NGT)患者中,使用 25、75 和 125 g 口服葡萄糖耐量试验(OGTT)和等血糖静脉内葡萄糖输注(IIGI)研究了胰岛素分泌的肠促胰岛素效应。使用嵌入剂量反应(斜率=葡萄糖敏感性)、早期反应(速率敏感性)和增强作用(与时间相关的分泌增加)的模型评估 β 细胞反应。对于每个参数,均计算了 OGTT/IIGI 比值的肠促胰岛素效应。在 NGT 中,肠促胰岛素对总分泌的作用随剂量增加(IIGI 的 1.3 ± 0.1、1.7 ± 0.2 和 2.2 ± 0.2 倍,P<0.0001),这是由剂量依赖性增加肠促胰岛素对葡萄糖敏感性的作用(1.9 ± 0.4、2.4 ± 0.4 和 3.1 ± 0.4,P=0.005)和剂量独立增强肠促胰岛素对速率敏感性的作用(894 [1145]、454 [516] 和 783 [1259] pmol m(-2) L mmol(-1)高于 IIGI;中位数[四分位距],P<0.0001)介导的。肠促胰岛素对增强作用也增加(0.97 ± 0.06、1.45 ± 0.20、1.24 ± 0.16,P<0.0001)。在 T2D 中,肠促胰岛素对总分泌(1.0 ± 0.1、1.1 ± 0.1 和 1.3 ± 0.1,P=0.004)和葡萄糖敏感性(1.2 ± 0.2、1.3 ± 0.2 和 2.0 ± 0.2,P=0.005)受损与 NGT;然而,在 25 g 时,肠促胰岛素对速率敏感性的作用已经增加(IIGI 以上的 269 [169]、284 [301] 和 193 [465] pmol m(-2) L mmol(-1);T2D 中几乎没有 IIGI 速率敏感性,无法计算倍数增加)。OGTT 没有在 IIGI 以上刺激增强作用(0.94 ± 0.04、0.89 ± 0.06 和 1.06 ± 0.09;P<0.01 与 NGT 相比)。在整个组中,尽管在 T2D 中系统降低,但肠促胰岛素作用与 IIGI 期间的总分泌呈负相关。总之,1)在 NGT 中,葡萄糖敏感性和增强作用介导了剂量依赖性肠促胰岛素作用增加;2)在 T2D 中,肠促胰岛素作用与 NGT 相比减弱,但在所有负荷下速率敏感性增强;3)NGT 中相对较低的肠促胰岛素作用与 IIGI 期间较高的分泌有关,这表明降低的肠促胰岛素作用不是由于β细胞功能障碍所致。