Campos Luciana Silveira, Limberger Leo Francisco, Stein Airton Tetelbom, Kalil Antonio Nocchi
Serviço de Ginecologia do Hospital Nossa Senhora da Conceição, Av Francisco Trein, 596, Bairro Cristo Redentor CEP, Porto Alegre 91350-200, Brazil.
Trials. 2013 Sep 12;14:293. doi: 10.1186/1745-6215-14-293.
Non-randomised studies have suggested that the postoperative complications of (Campos LS, Limberger LF, Stein AT, Kalil AN) laparoscopic radical hysterectomy are similar to those in abdominal radical hysterectomy. However, no study evaluating postoperative pain comparing both techniques has been published thus far. Our objective was to compare pain intensity and other perioperative outcomes between laparoscopic radical hysterectomy (LRH) and abdominal radical hysterectomy (ARH) in early cervical cancer.
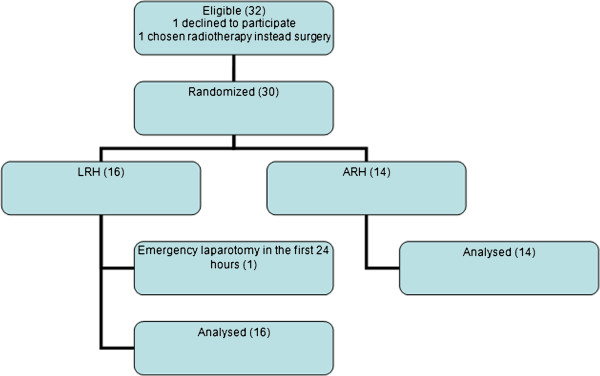
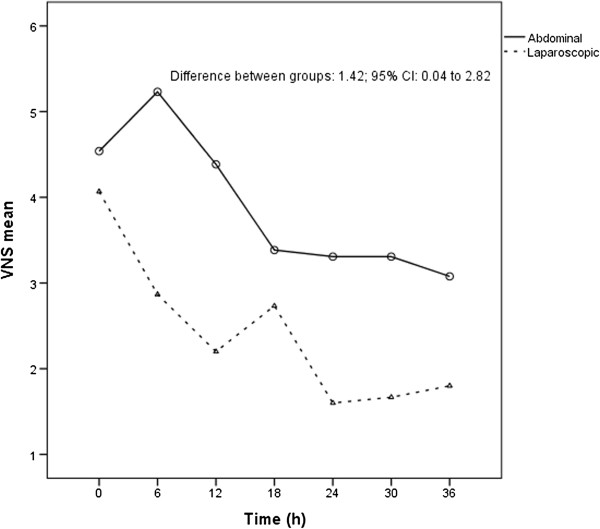
This single centre, randomised, controlled trial enrolled 30 cervical cancer patients who were clinically staged IA2 with lymph vascular invasion and IB according to the FIGO (International Federation of Gynaecology and Obstetrics) classification, and underwent LRH or ARH between late 1999 and early 2004. Postoperative pain, as measured by a 10-point numerical rate scale, was considered the primary endpoint. Postoperative pain was assessed every six hours during a patient's usual postoperative care. Perioperative outcomes were also registered. Both surgical techniques were executed by the same surgical team. Secondary outcomes included intraoperative and other postoperative surgicopathological factors and 5-year survival rates.
IA2 patients with lymphatic vascular space invasion and IB cervical cancer patients were randomised to either the LRH group (16 patients) or the ARH group (14 patients). Four patients (25%) in the LRH group and 5 patients (36%) in the ARH group presented with transoperative or serious postoperative complications. All of the transoperative complications occurred in the LRH group. The relative risk of presenting with complications was 0.70; CI 95% (0.23-2.11); P = 0.694. LRH group mean pain score was significantly lower than ARH after 36 h of observation (P = 0.044; mean difference score: 1.42; 95% CI: 0.04-2.80). The survival results will be published elsewhere.
LRH provided lower pain scores after 36 h of observation in this series. The perioperative and serious postoperative complications ratios were comparable between the groups.
NCT01258413.
非随机研究表明,(坎波斯LS、林伯格LF、斯坦因AT、卡利尔AN)腹腔镜根治性子宫切除术的术后并发症与腹式根治性子宫切除术相似。然而,迄今为止,尚无评估这两种技术术后疼痛情况的研究发表。我们的目的是比较早期宫颈癌患者腹腔镜根治性子宫切除术(LRH)和腹式根治性子宫切除术(ARH)的疼痛强度及其他围手术期结局。
这项单中心、随机、对照试验纳入了30例宫颈癌患者,根据国际妇产科联盟(FIGO)分类,这些患者临床分期为IA2期伴淋巴血管浸润和IB期,并于1999年末至2004年初接受了LRH或ARH手术。以10分数字评分量表测量的术后疼痛被视为主要终点。在患者常规术后护理期间,每6小时评估一次术后疼痛。还记录围手术期结局。两种手术技术均由同一手术团队实施。次要结局包括术中及其他术后手术病理因素和5年生存率。
IA2期伴淋巴血管间隙浸润的患者和IB期宫颈癌患者被随机分为LRH组(16例患者)或ARH组(14例患者)。LRH组有4例患者(25%)出现术中或严重术后并发症,ARH组有5例患者(36%)出现此类情况。所有术中并发症均发生在LRH组。出现并发症的相对风险为0.70;95%置信区间(0.23 - 2.11);P = 0.694。观察36小时后,LRH组的平均疼痛评分显著低于ARH组(P = 0.044;平均差异评分:1.42;95%置信区间:0.04 - 2.80)。生存结果将在其他地方发表。
在本系列研究中,观察36小时后LRH的疼痛评分较低。两组的围手术期及严重术后并发症发生率相当。
NCT01258413。