Pitta Denise da Rocha, Sarian Luis Otávio, Barreta Amilcar, Campos Elisabete Aparecida, Andrade Liliana Lucci de Angelo, Fachini Ana Maria Dias, Campbell Leonardo Martins, Derchain Sophie
Department of Obstetrics and Gynecology, Faculty of Medical Sciences, State University of Campinas - Unicamp, Campinas, SP 13083-970, Brazil.
BMC Cancer. 2013 Sep 18;13:423. doi: 10.1186/1471-2407-13-423.
This manuscript evaluates whether specific symptoms, a symptom index (SI), CA125 and HE4 can help identify women with malignant tumors in the group of women with adnexal masses previously diagnosed with ultrasound.
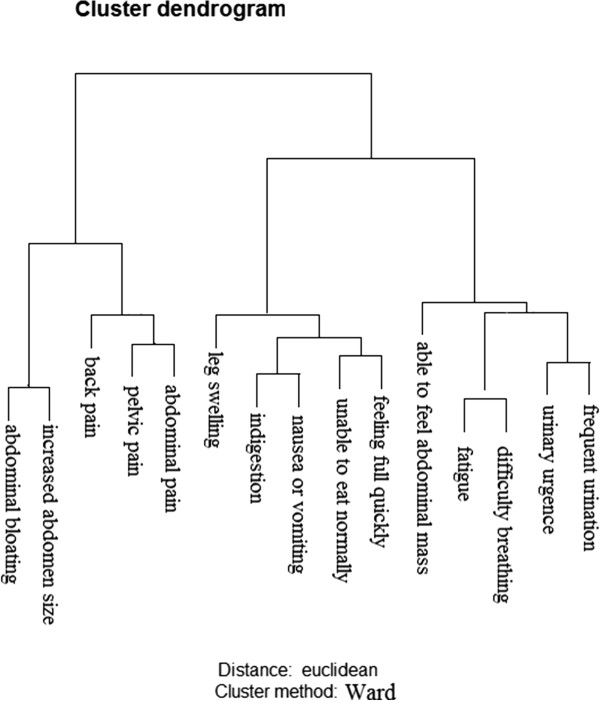
This was a cross-sectional study with data collection between January 2010 and January 2012. We invited 176 women with adnexal masses of suspected ovarian origin, attending the hospital of the Department of Obstetrics and Gynecology of the Unicamp School of Medicine. A control group of 150 healthy women was also enrolled. Symptoms were assessed with a questionnaire tested previously. Women with adnexal masses were interviewed before surgery to avoid recall bias. The Ward Agglomerative Method was used to define symptom clusters. Serum measurements of CA125 and HE4 were made. The Risk of Ovarian Malignancy Algorithm (ROMA) was calculated using standard formulae.
Sixty women had ovarian cancer and 116 benign ovarian tumors. Six symptom clusters were formed and three specific symptoms (back pain, leg swelling and able to feel abdominal mass) did not agglomerate. A symptom index (SI) using clusters abdomen, pain and eating was formed. The sensitivity of the SI in discriminating women with malignant from those with benign ovarian tumors was 78.3%, with a specificity of 60.3%. Positive SI was more frequent in women with malignant than in women with benign tumors (OR 5.5; 95% CI 2.7 to 11.3). Elevated CA125 (OR 11.8; 95% CI 5.6 to 24.6) or HE4 (OR 7.6; 95% CI 3.7 to 15.6) or positive ROMA (OR 9.5; 95% CI 4.4 to 20.3) were found in women with malignant tumors compared with women with benign tumors. The AUC-ROC for CA125 was not different from that for HE4 or ROMA. The best specificity and negative predictive values were obtained using CA125 in women with negative SI.
Women diagnosed with an adnexal mass could benefit from a short enquiry about presence, frequency and onset of six symptoms, and CA125 measurements. Primary care physicians can be thereby assisted in deciding as to whether or not reference the woman to often busy, congested specialized oncology centers.
本论文评估特定症状、症状指数(SI)、CA125和HE4能否帮助在先前经超声诊断为附件包块的女性群体中识别出患有恶性肿瘤的女性。
这是一项横断面研究,于2010年1月至2012年1月期间收集数据。我们邀请了176名怀疑卵巢来源附件包块的女性,她们前往坎皮纳斯医学院妇产科医院就诊。还纳入了150名健康女性作为对照组。症状通过先前测试过的问卷进行评估。对附件包块女性在手术前进行访谈以避免回忆偏倚。采用沃德凝聚法定义症状群。进行CA125和HE4的血清检测。使用标准公式计算卵巢恶性肿瘤风险算法(ROMA)。
60名女性患有卵巢癌,116名患有良性卵巢肿瘤。形成了六个症状群,三个特定症状(背痛、腿部肿胀和能摸到腹部包块)未聚集。形成了一个使用腹部、疼痛和饮食群的症状指数(SI)。SI区分恶性卵巢肿瘤女性和良性卵巢肿瘤女性的敏感性为78.3%,特异性为60.3%。SI阳性在恶性肿瘤女性中比在良性肿瘤女性中更常见(比值比5.5;95%置信区间2.7至11.3)。与良性肿瘤女性相比,恶性肿瘤女性中CA125升高(比值比11.8;95%置信区间5.6至24.6)或HE4升高(比值比7.6;95%置信区间3.7至15.6)或ROMA阳性(比值比9.5;95%置信区间4.4至20.3)。CA125的曲线下面积(AUC-ROC)与HE4或ROMA的无差异。在SI阴性的女性中使用CA125可获得最佳特异性和阴性预测值。
被诊断为附件包块的女性可通过简短询问六种症状的存在、频率和发作情况以及进行CA125检测而受益。初级保健医生因此可得到帮助,以决定是否将该女性转诊至通常繁忙、拥挤的专科肿瘤中心。