Fraser Chris, Brown Patrick, Megason Gail, Ahn Hyo Seop, Cho Bin, Kirov Ivan, Frankel Lawrence, Aplenc Richard, Bensen-Kennedy Debra, Munteanu Mihaela, Weaver Jennifer, Harker-Murray Paul
*Royal Children's Hospital, Brisbane, Qld, Australia †Johns Hopkins University School of Medicine, Baltimore, MD ‡University of Mississippi, Jackson, MS §Cancer Research Institute, Seoul National University College of Medicine ∥The Catholic University of Korea, Seoul, Republic of Korea ¶CHOC Children's, Orange, CA #Pharmaceutical Product Development Inc., Wilmington, NC **The Children's Hospital of Philadelphia, Philadelphia, PA ††CSL Behring, King of Prussia, PA (formerly of Cephalon Inc., which is now a wholly owned subsidiary of Teva Branded Pharmaceutical Products R&D Inc., Frazer, PA) ‡‡Teva Branded Pharmaceutical Products R&D Inc., Frazer, PA §§CSL Behring, King of Prussia, PA (formerly of Teva Branded Pharmaceutical Products R&D Inc., Frazer, PA) ∥∥Southwestern Medical Center, University of Texas, Dallas, TX.
J Pediatr Hematol Oncol. 2014 May;36(4):e212-8. doi: 10.1097/MPH.0000000000000021.
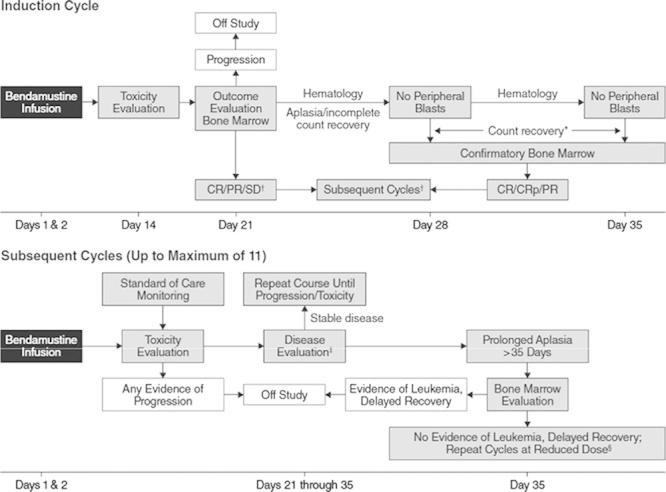
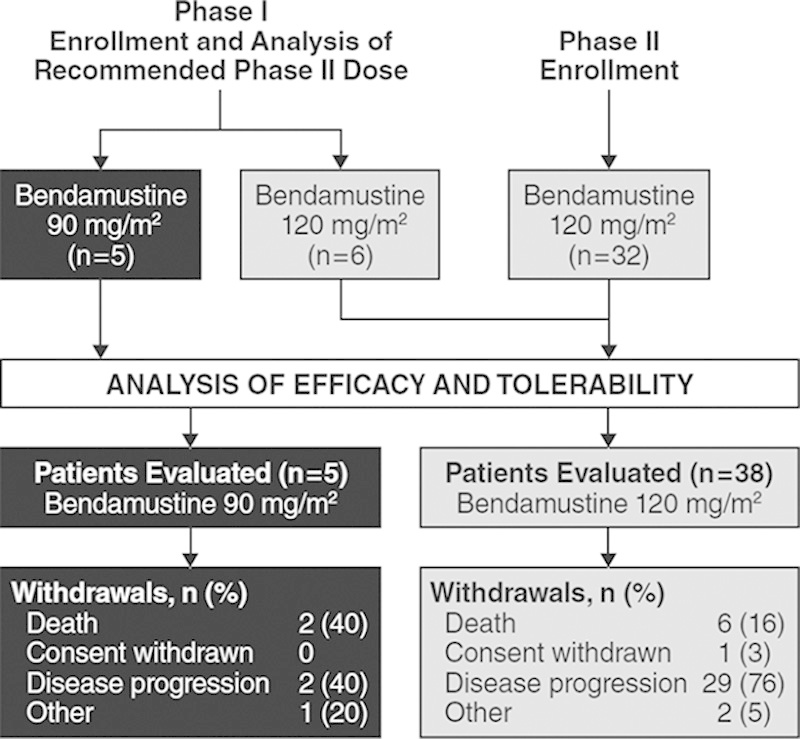
This open-label, single-arm, phase I/II, dose-escalation study was designed to determine the recommended phase II dose (RP2D), pharmacokinetics, tolerability, and efficacy of bendamustine in pediatric patients (age ranging from 1 to 20 y) with histologically proven relapsed/refractory acute lymphoblastic leukemia (ALL) or acute myeloid leukemia (AML). Patients (27 with ALL, 16 with AML) received intravenous bendamustine on days 1 and 2 of each treatment cycle. Phase I involved planned dose escalation of bendamustine to establish the RP2D for phase II. Objectives included overall response rate, duration of response, and tolerability. Eleven patients were treated in phase I, and the RP2D was 120 mg/m. In phase II, 32 patients received bendamustine 120 mg/m. Two patients with ALL (bendamustine 90 mg/m) experienced complete response (CR). Among patients who received bendamustine 120 mg/m, 2 experienced partial response (PR); 7 had stable disease. The overall response rate (CR+CR without platelet recovery [CRp]) was 4.7% and biological activity rate (CR+CRp+PR) was 9.3%. No AML patients responded. The most common adverse events were anemia, neutropenia, thrombocytopenia, pyrexia, nausea, vomiting, and diarrhea. Bendamustine monotherapy has acceptable tolerability in heavily pretreated children with relapsed/refractory ALL or AML and appears to have some activity in ALL, warranting further studies in combination trials.
这项开放标签、单臂、I/II期剂量递增研究旨在确定苯达莫司汀在组织学确诊为复发/难治性急性淋巴细胞白血病(ALL)或急性髓系白血病(AML)的儿科患者(年龄1至20岁)中的推荐II期剂量(RP2D)、药代动力学、耐受性和疗效。患者(27例ALL,16例AML)在每个治疗周期的第1天和第2天接受静脉注射苯达莫司汀。I期包括计划的苯达莫司汀剂量递增,以确定II期的RP2D。目标包括总缓解率、缓解持续时间和耐受性。11例患者接受了I期治疗,RP2D为120mg/m²。在II期,32例患者接受120mg/m²的苯达莫司汀治疗。2例ALL患者(苯达莫司汀90mg/m²)出现完全缓解(CR)。在接受120mg/m²苯达莫司汀治疗的患者中,2例出现部分缓解(PR);7例病情稳定。总缓解率(CR+未恢复血小板的CR[CRp])为4.7%,生物学活性率(CR+CRp+PR)为9.3%。无AML患者有反应。最常见的不良事件是贫血、中性粒细胞减少、血小板减少、发热、恶心、呕吐和腹泻。苯达莫司汀单药治疗在复发/难治性ALL或AML的重度预处理儿童中具有可接受的耐受性,并且在ALL中似乎有一定活性,值得在联合试验中进一步研究。