Ghotbi Adam Ali, Køber Lars, Finer Nick, James W Philip T, Sharma Arya M, Caterson Ian, Coutinho Walmir, Van Gaal Luc F, Torp-Pedersen Christian, Andersson Charlotte
Corresponding author: Adam Ali Ghotbi,
Diabetes Care. 2013 Nov;36(11):3746-53. doi: 10.2337/dc13-0027. Epub 2013 Oct 2.
To assess the association of hypoglycemic treatment regimens with cardiovascular adverse events and mortality in a large population of type 2 diabetic patients at increased cardiovascular risk.
This analysis included 8,192 overweight patients with type 2 diabetes from the Sibutramine Cardiovascular Outcomes (SCOUT) trial randomized to lifestyle intervention with or without sibutramine for up to 6 years. Patients were grouped according to hypoglycemic treatment at baseline. The primary end point was the time from randomization to the first occurrence of a primary outcome event (POE), nonfatal myocardial infarction, nonfatal stroke, resuscitation after cardiac arrest, or cardiovascular death. Multivariable Cox proportional hazards regression models were used to assess the impact of antiglycemic treatment on POE and all-cause mortality.
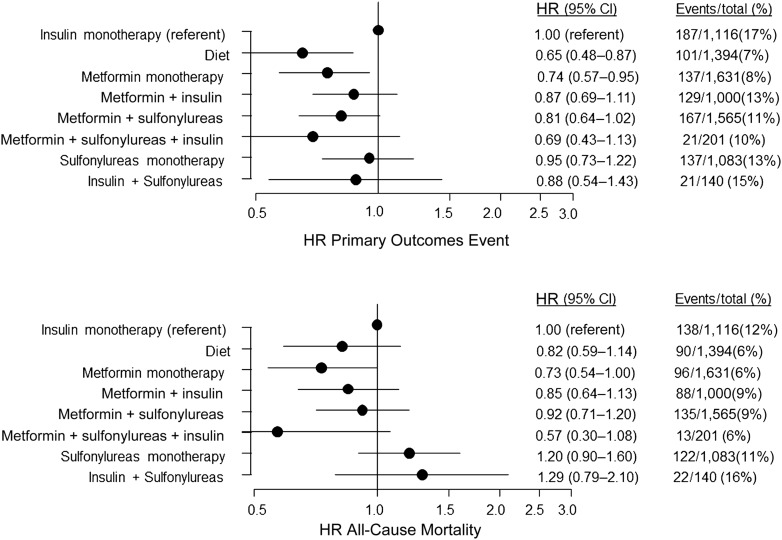
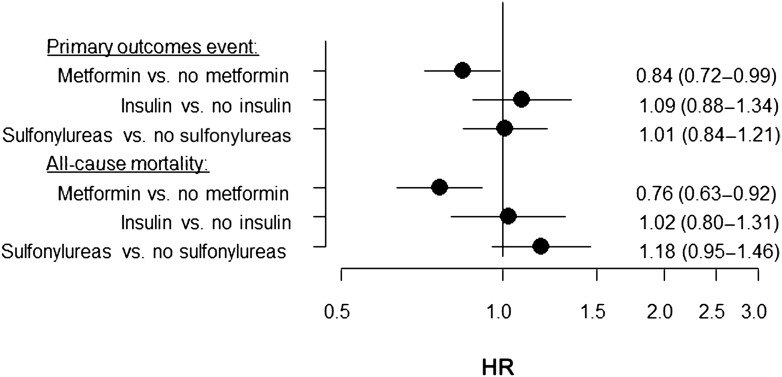
Treatments for type 2 diabetes were as follows: diet alone (n = 1,394 subjects), metformin monotherapy (n = 1,631), insulin monotherapy (n = 1,116), sulfonylurea monotherapy (n = 1,083), metformin plus sulfonylurea (n = 1,565), and metformin plus insulin (n = 1,000); 905 subjects experienced a POE and 708 died. Metformin monotherapy was associated with lower risk of POE than insulin (hazard ratio [HR], 0.74; 95% CI, 0.57-0.95; P = 0.02). Diet alone also was associated with lower risk of POE (HR, 0.65; 95% CI, 0.48-0.87; P = 0.004). Metformin monotherapy also was associated with lower mortality (HR, 0.73; 95% CI, 0.54-0.99; P < 0.05), whereas no other monotherapies or combination therapies were significantly associated with POE or all-cause mortality compared with insulin as monotherapy.
In obese patients with type 2 diabetes and high risk of cardiovascular disease, monotherapy with metformin or diet-only treatment was associated with lower risk of cardiovascular events than treatment with insulin.
评估在心血管疾病风险增加的2型糖尿病患者大群体中,降糖治疗方案与心血管不良事件及死亡率之间的关联。
该分析纳入了来自西布曲明心血管结局(SCOUT)试验的8192例超重2型糖尿病患者,这些患者被随机分配接受长达6年的生活方式干预,部分患者联合使用或不使用西布曲明。患者根据基线时的降糖治疗进行分组。主要终点是从随机分组到首次发生主要结局事件(POE)、非致命性心肌梗死、非致命性中风、心脏骤停复苏或心血管死亡的时间。使用多变量Cox比例风险回归模型来评估降糖治疗对POE和全因死亡率的影响。
2型糖尿病的治疗方式如下:单纯饮食治疗(n = 1394例受试者)、二甲双胍单药治疗(n = 1631例)、胰岛素单药治疗(n = 1116例)、磺脲类药物单药治疗(n = 1083例)、二甲双胍加磺脲类药物(n = 1565例)以及二甲双胍加胰岛素(n = 1000例);905例受试者发生了POE,708例死亡。二甲双胍单药治疗与POE风险低于胰岛素治疗相关(风险比[HR],0.74;95%可信区间[CI],0.57 - 0.95;P = 0.02)。单纯饮食治疗也与较低的POE风险相关(HR,0.65;95% CI,0.48 - 0.87;P = 0.004)。二甲双胍单药治疗还与较低的死亡率相关(HR,0.73;95% CI,0.54 - 0.99;P < 0.05),而与胰岛素单药治疗相比,没有其他单药治疗或联合治疗与POE或全因死亡率显著相关。
在患有2型糖尿病且心血管疾病风险高的肥胖患者中,与胰岛素治疗相比,二甲双胍单药治疗或单纯饮食治疗与较低的心血管事件风险相关。