Princess Amalia Children's Centre, Isala hospital, PO Box 10400, 8000 GK, Zwolle, the Netherlands.
Clin Transl Allergy. 2013 Oct 10;3(1):34. doi: 10.1186/2045-7022-3-34.
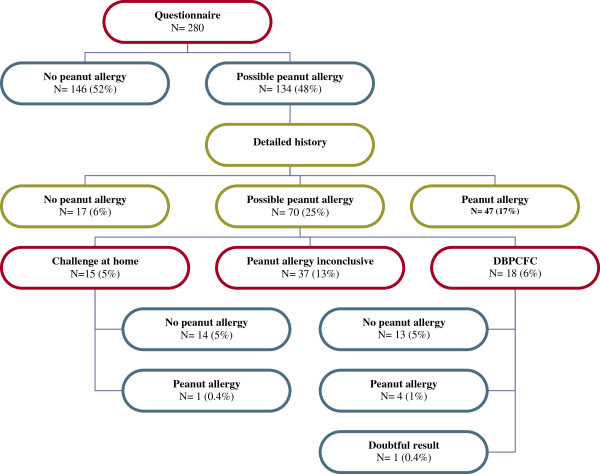
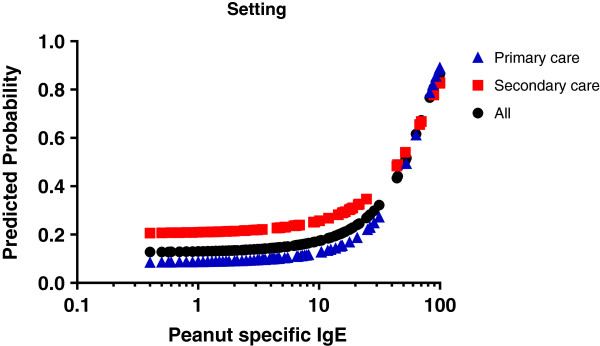
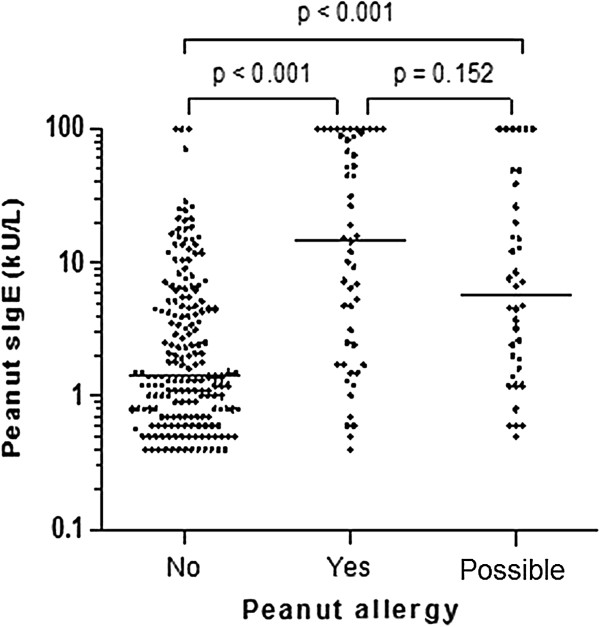
The usefulness of peanut specific IgE levels for diagnosing peanut allergy has not been studied in primary and secondary care where most cases of suspected peanut allergy are being evaluated. We aimed to determine the relationship between peanut-specific IgE levels and clinical peanut allergy in peanut-sensitized children and how this was influenced by eczema, asthma and clinical setting (primary or secondary care). We enrolled 280 children (0-18 years) who tested positive for peanut-specific IgE (> 0.35 kU/L) requested by primary and secondary physicians. We used predefined criteria to classify participants into three groups: peanut allergy, no peanut allergy, or possible peanut allergy, based on responses to a validated questionnaire, a detailed food history, and results of oral food challenges.Fifty-two participants (18.6%) were classified as peanut allergy, 190 (67.9%) as no peanut allergy, and 38 (13.6%) as possible peanut allergy. The association between peanut-specific IgE levels and peanut allergy was significant but weak (OR 1.46 for a 10.0 kU/L increase in peanut-specific IgE, 95% CI 1.28-1.67). Eczema was the strongest risk factor for peanut allergy (aOR 3.33, 95% CI 1.07-10.35), adjusted for demographic and clinical characteristics. Asthma was not significantly related to peanut allergy (aOR 1.93, 95% CI 0.90-4.13). Peanut allergy was less likely in primary than in secondary care participants (OR 0.46, 95% CI 0.25-0.86), at all levels of peanut-specific IgE.The relationship between peanut-specific IgE and peanut allergy in children is weak, is strongly dependent on eczema, and is weaker in primary compared to secondary care. This limits the usefulness of peanut-specific IgE levels in the diagnosis of peanut allergy in children.
花生特异性 IgE 水平在初级和二级保健中用于诊断花生过敏的作用尚未得到研究,而大多数疑似花生过敏的病例都在这些地方进行评估。我们旨在确定花生致敏儿童中花生特异性 IgE 水平与临床花生过敏之间的关系,以及特应性皮炎、哮喘和临床环境(初级或二级保健)对此的影响。我们招募了 280 名(0-18 岁)经初级和二级医生要求检测花生特异性 IgE(>0.35 kU/L)呈阳性的儿童。我们使用预定义的标准,根据一份经过验证的问卷、详细的食物史和口服食物挑战的结果,将参与者分为三组:花生过敏、无花生过敏或可能的花生过敏。52 名参与者(18.6%)被归类为花生过敏,190 名(67.9%)为无花生过敏,38 名(13.6%)为可能的花生过敏。花生特异性 IgE 水平与花生过敏之间存在显著但较弱的关联(花生特异性 IgE 每增加 10.0 kU/L,花生过敏的比值比为 1.46,95%CI 为 1.28-1.67)。特应性皮炎是花生过敏的最强危险因素(调整人口统计学和临床特征后的优势比为 3.33,95%CI 为 1.07-10.35)。哮喘与花生过敏无显著相关性(比值比为 1.93,95%CI 为 0.90-4.13)。与二级保健参与者相比,初级保健参与者的花生过敏可能性更低(比值比为 0.46,95%CI 为 0.25-0.86),且在所有花生特异性 IgE 水平下均如此。儿童中花生特异性 IgE 与花生过敏之间的关系较弱,强烈依赖于特应性皮炎,在初级保健中比在二级保健中更弱。这限制了花生特异性 IgE 水平在儿童花生过敏诊断中的作用。