Offman Elliot, Marenco Ted, Ferber Sandy, Johnson Judith, Kling Douglas, Curcio Danielle, Davidson Michael
Clinical Pharmacology Sciences, Celerion, Montreal, QC, Canada.
Vasc Health Risk Manag. 2013;9:563-73. doi: 10.2147/VHRM.S50464. Epub 2013 Oct 1.
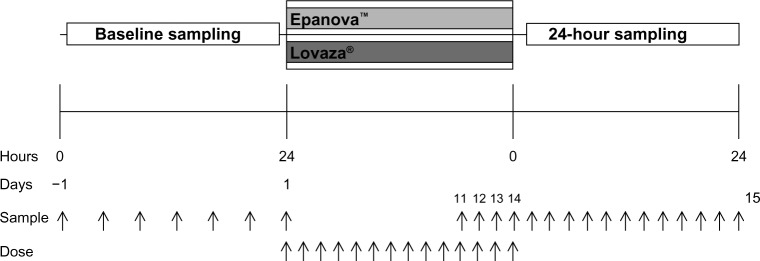
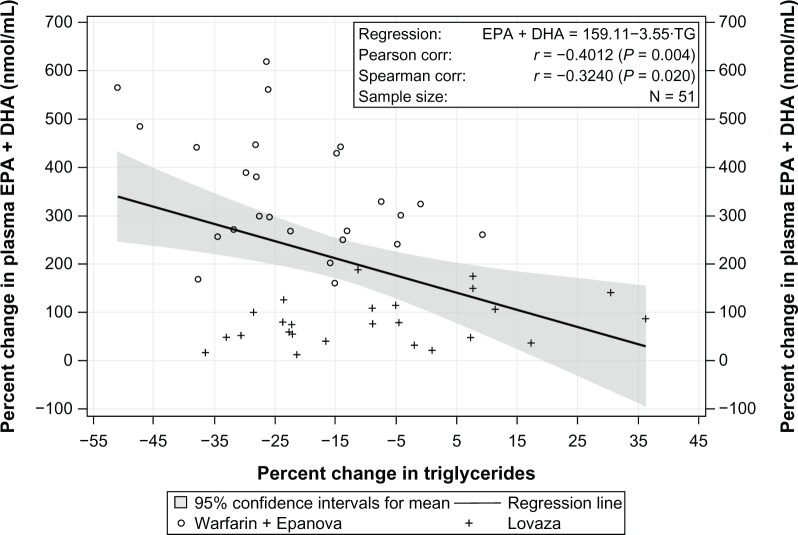
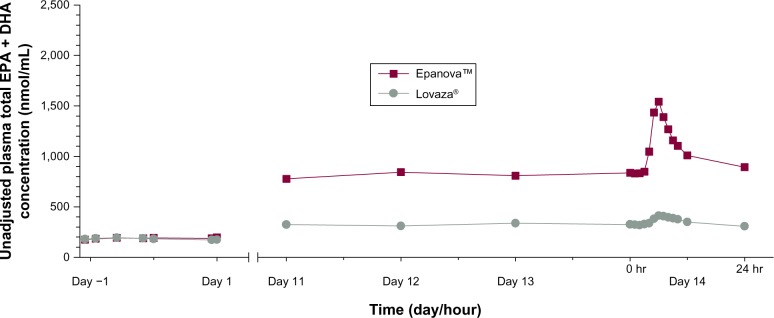
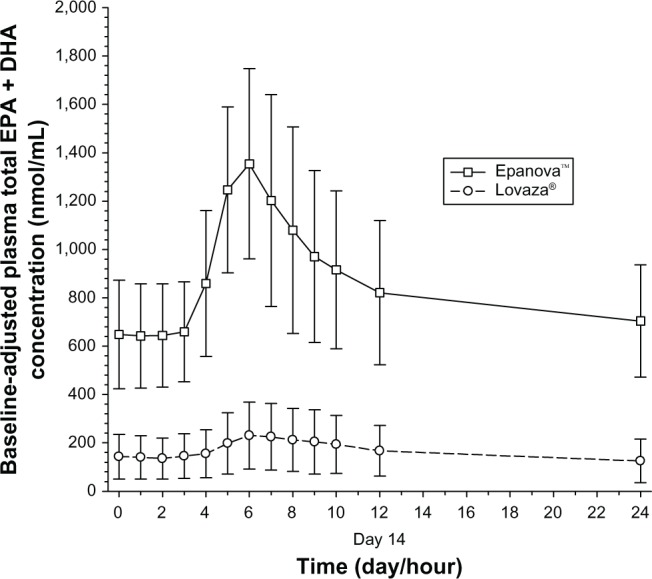
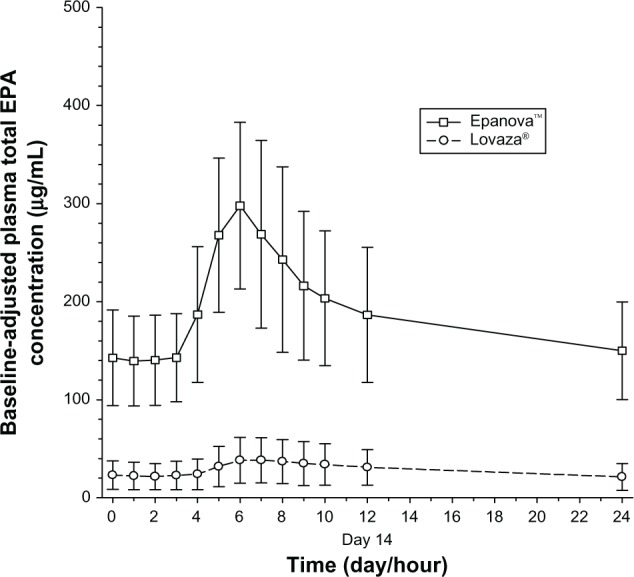
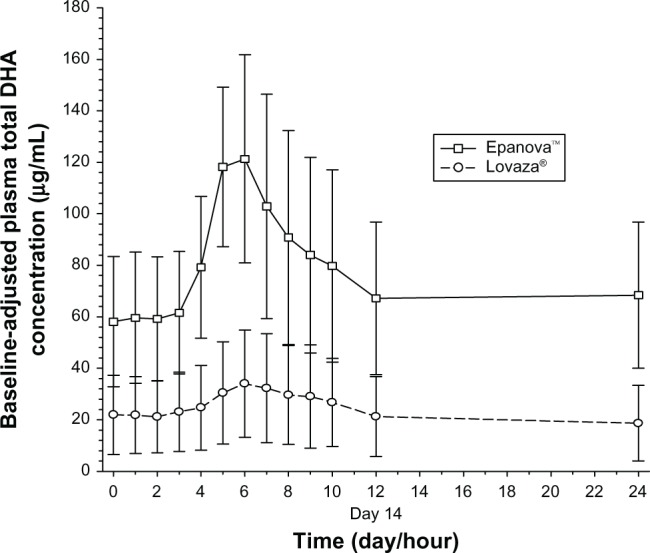
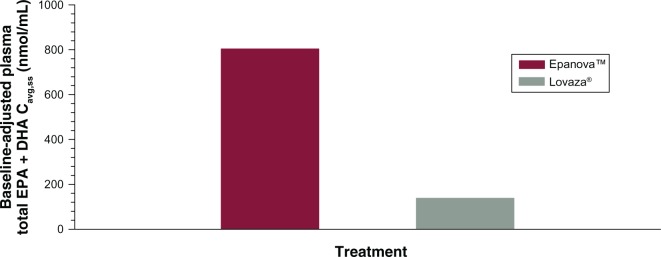
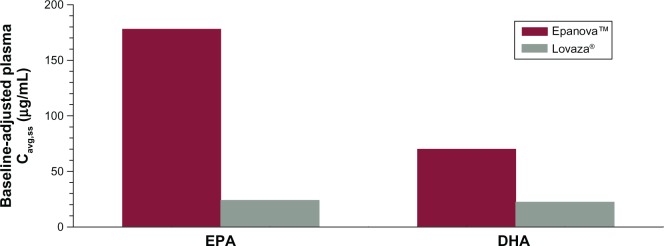
The systemic bioavailability of free fatty acid (FFA) forms of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) compared with ethyl ester (EE) forms is dependent on the presence of intestinal lipases and is highest during consumption of high-fat meals. Given that patients with cardiovascular disease are advised to reduce dietary fat intake, potentially lowering the bioavailability and therapeutic benefit, the hypothesis that FFA forms provide for higher bioavailability compared with EE forms under low-fat diet conditions was tested where the pharmacokinetics of the FFA form (Epanova™) were compared with those of an ethyl ester form (Lovaza®) following repeat dosing. Fifty-two healthy male and female subjects were equally allocated to one of two open-label, parallel-group cohorts. Following a Therapeutic Lifestyle Changes diet for a minimum of 7 days, blood samples were drawn for endogenous values for EPA and DHA over a 24-hour period. Subjects were then administered 4 × 1 g capsules of either Epanova (OM3 FFA) or Lovaza (OM3 EE) once daily for 14 days, following which serial blood samples were drawn over a 24-hour period to characterize the bioavailability of EPA and DHA from the respective formulations. In addition, changes from baseline in lipid profile were explored. Systemic bioavailability, as measured by area under the curve from time zero to 24 hours (AUC(0-τ)) and the maximum measured plasma concentrations during the 0-24 hour dosing interval (C(max,ss)) of unadjusted total plasma EPA + DHA were approximately 3-fold and 3.9-fold higher, respectively, for Epanova relative to Lovaza. Following baseline adjustment, the magnitude of difference in bioavailability was approximately 5.8-fold and 6.5-fold higher in AUC(0-τ) and C(max,ss), respectively, for Epanova relative to Lovaza. Serum triglycerides were reduced by a significantly greater extent (P = 0.013) for Epanova relative to Lovaza (21% versus 8%). The bioavailability of the FFA forms of EPA and DHA in Epanova are significantly greater than the bioavailability from the EE forms present in Lovaza under low-fat dietary conditions normally recommended for patients with cardiovascular disease. This increased bioavailability may lead to improved triglyceride-lowering in patients with hypertriglyceridemia.
与二十碳五烯酸(EPA)和二十二碳六烯酸(DHA)的乙酯(EE)形式相比,游离脂肪酸(FFA)形式的全身生物利用度取决于肠道脂肪酶的存在,并且在高脂餐食用期间最高。鉴于建议心血管疾病患者减少膳食脂肪摄入,这可能会降低生物利用度和治疗益处,因此对以下假设进行了测试:在低脂饮食条件下,FFA形式比EE形式具有更高的生物利用度,其中在重复给药后将FFA形式(Epanova™)的药代动力学与乙酯形式(Lovaza®)的药代动力学进行比较。52名健康男性和女性受试者被平均分配到两个开放标签、平行组队列之一。在遵循治疗性生活方式改变饮食至少7天后,在24小时内采集血样以获取EPA和DHA的内源性值。然后,受试者每天服用4粒1克胶囊的Epanova(OM3 FFA)或Lovaza(OM3 EE),持续14天,之后在24小时内采集系列血样以表征各自制剂中EPA和DHA的生物利用度。此外,还探讨了血脂谱相对于基线的变化。以从零到24小时的曲线下面积(AUC(0-τ))和0-24小时给药间隔期间测得的最大血浆浓度(C(max,ss))衡量,Epanova的未调整总血浆EPA + DHA的全身生物利用度分别比Lovaza高约3倍和3.9倍。经过基线调整后,Epanova相对于Lovaza的AUC(0-τ)和C(max,ss)的生物利用度差异幅度分别高约5.8倍和6.5倍。相对于Lovaza,Epanova使血清甘油三酯降低的程度明显更大(P = 0.013)(21%对8%)。在通常推荐给心血管疾病患者的低脂饮食条件下,Epanova中EPA和DHA的FFA形式的生物利用度明显高于Lovaza中EE形式的生物利用度。这种增加的生物利用度可能会改善高甘油三酯血症患者的甘油三酯降低情况。