Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland, United States of America.
PLoS Med. 2013 Oct;10(10):e1001524. doi: 10.1371/journal.pmed.1001524. Epub 2013 Oct 1.
Oxytocin (10 IU) is the drug of choice for prevention of postpartum hemorrhage (PPH). Its use has generally been restricted to medically trained staff in health facilities. We assessed the effectiveness, safety, and feasibility of PPH prevention using oxytocin injected by peripheral health care providers without midwifery skills at home births.
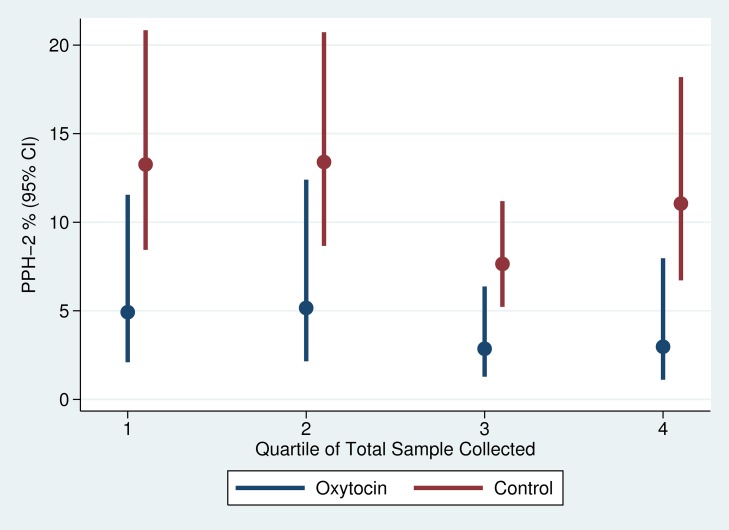
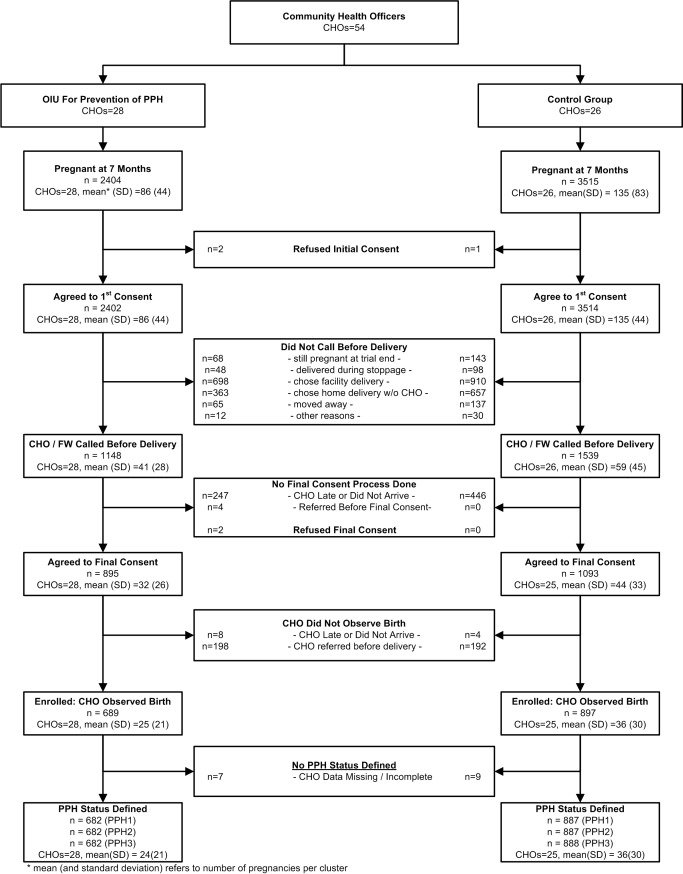
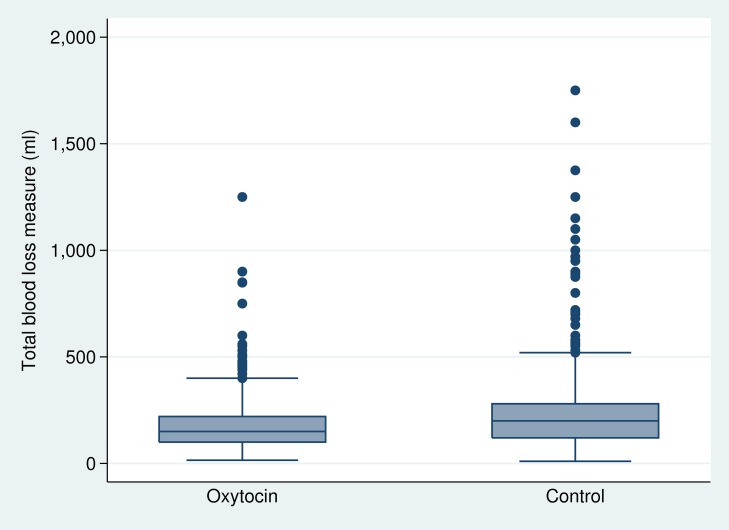
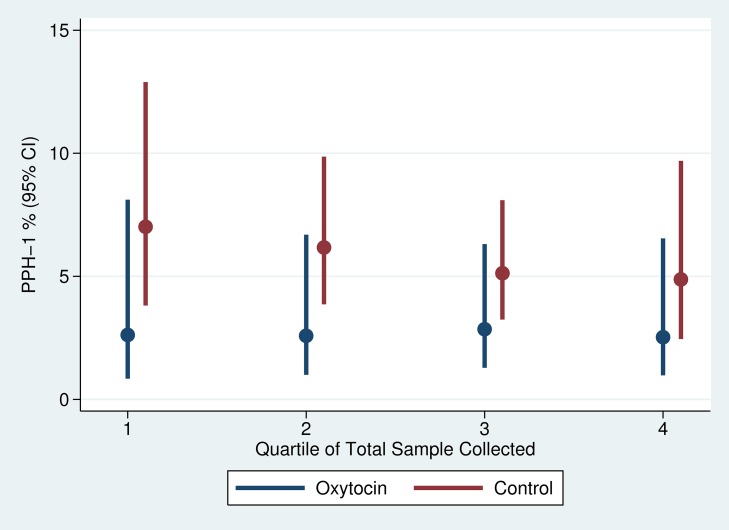
This community-based, cluster-randomized trial was conducted in four rural districts in Ghana. We randomly allocated 54 community health officers (stratified on district and catchment area distance to a health facility: ≥10 km versus <10 km) to intervention (one injection of oxytocin [10 IU] one minute after birth) and control (no provision of prophylactic oxytocin) arms. Births attended by a community health officer constituted a cluster. Our primary outcome was PPH, using multiple definitions; (PPH-1) blood loss ≥500 mL; (PPH-2) PPH-1 plus women who received early treatment for PPH; and (PPH-3) PPH-2 plus any other women referred to hospital for postpartum bleeding. Unsafe practice is defined as oxytocin use before delivery of the baby. We enrolled 689 and 897 women, respectively, into oxytocin and control arms of the trial from April 2011 to November 2012. In oxytocin and control arms, respectively, PPH-1 rates were 2.6% versus 5.5% (RR: 0.49; 95% CI: 0.27-0.88); PPH-2 rates were 3.8% versus 10.8% (RR: 0.35; 95% CI: 0.18-0.63), and PPH-3 rates were similar to those of PPH-2. Compared to women in control clusters, those in the intervention clusters lost 45.1 mL (17.7-72.6) less blood. There were no cases of oxytocin use before delivery of the baby and no major adverse events requiring notification of the institutional review boards. Limitations include an unblinded trial and imbalanced numbers of participants, favoring controls.
Maternal health care planners can consider adapting this model to extend the use of oxytocin into peripheral settings including, in some contexts, home births.
ClinicalTrials.gov NCT01108289 Please see later in the article for the Editors' Summary.
缩宫素(10IU)是预防产后出血(PPH)的首选药物。其使用通常限于医疗机构中接受过医学培训的人员。我们评估了在家分娩时,由缺乏助产技能的基层医疗保健提供者注射缩宫素预防 PPH 的效果、安全性和可行性。
这是一项在加纳四个农村地区进行的基于社区的集群随机试验。我们将 54 名社区卫生官员(按区和到卫生设施的集水区距离分层:≥10km 与 <10km)随机分配到干预(分娩后一分钟注射 1 次缩宫素[10IU])和对照(不提供预防性缩宫素)组。由社区卫生官员接生的分娩构成一个集群。我们的主要结局是使用多种定义的 PPH,包括(PPH-1)出血量≥500mL;(PPH-2)PPH-1 加产后出血早期接受治疗的妇女;以及(PPH-3)PPH-2 加任何因产后出血而转往医院的妇女。不安全的做法定义为在婴儿出生前使用缩宫素。我们分别于 2011 年 4 月至 2012 年 11 月,在缩宫素和对照组中,分别纳入了 689 名和 897 名妇女。在缩宫素和对照组中,PPH-1 的发生率分别为 2.6%和 5.5%(RR:0.49;95%CI:0.27-0.88);PPH-2 的发生率分别为 3.8%和 10.8%(RR:0.35;95%CI:0.18-0.63),PPH-3 的发生率与 PPH-2 相似。与对照组集群中的妇女相比,干预集群中的妇女失血减少了 45.1mL(17.7-72.6)。没有在婴儿出生前使用缩宫素的病例,也没有需要向机构审查委员会报告的重大不良事件。局限性包括试验未设盲以及参与者人数不平衡,对对照组有利。
产妇保健规划者可以考虑将这种模式应用于外围环境,包括在某些情况下,在家分娩时扩大缩宫素的使用。
ClinicalTrials.gov NCT01108289 请稍后在文章中查看编辑总结。