Jung Boris, Molinari Nicolas, Nasri Mourad, Hajjej Zied, Chanques Gerald, Jean-Pierre Helene, Panaro Fabrizio, Jaber Samir
Crit Care. 2013 Oct 24;17(5):R255. doi: 10.1186/cc13082.
Procalcitonin (PCT) biomarker is suggested to tailor antibiotic therapy in the medical intensive care unit (ICU) but studies in perioperative medicine are scarce. The aim of this study was to determine whether PCT reported thresholds are associated with the initial treatment response in perioperative septic shock secondary to intra-abdominal infection.
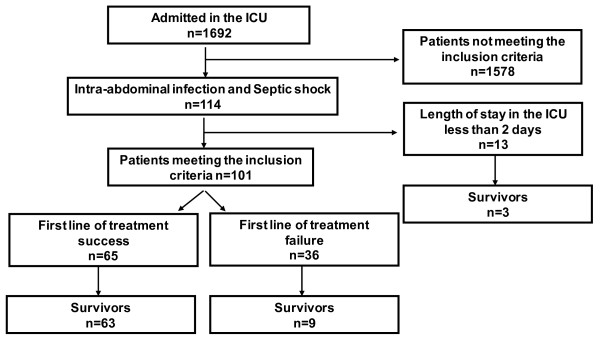
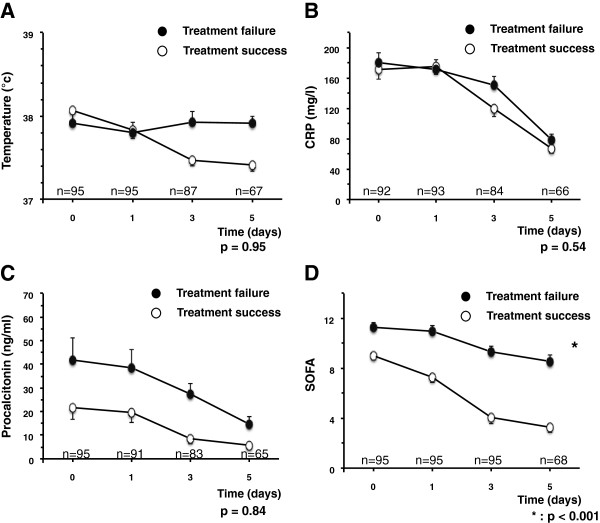
This single ICU, observational study included patients with perioperative septic shocks secondary to intra-abdominal infection. Demographics, PCT at days 0, 1, 3, 5, treatment response and outcome were collected. Treatment failure included death related to the initial infection, second source control treatment or a new onset intra-abdominal infection. The primary endpoint was to assess whether PCT thresholds (0.5 ng/ml or a drop from the peak of at least 80%) predict the initial treatment response.
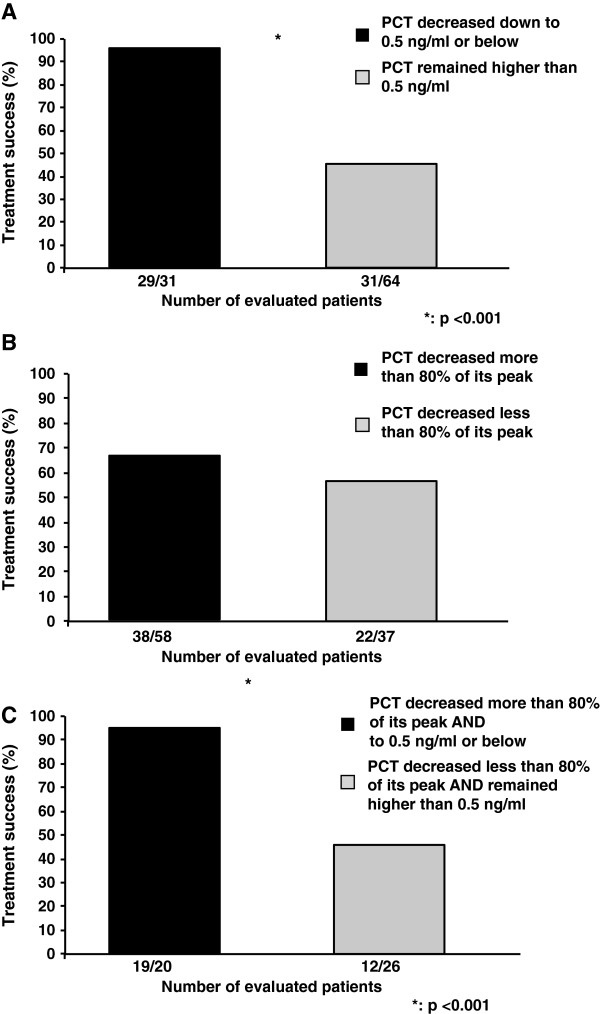
We included 101 consecutive cases. Initial treatment failed in 36 patients with a subsequent mortality of 75%. Upon admission, PCT was doubled when treatment ultimately failed (21.7 ng/ml ± 38.7 vs. 41.7 ng/ml ± 75.7; P = 0.04). Although 95% of the patients in whom PCT dropped down below 0.5 ng/ml responded to treatment, 50% of the patients in whom PCT remained above 0.5 ng/ml also responded successfully to treatment. Moreover, despite a PCT drop of at least 80%, 40% of patients had treatment failure.
In perioperative intra-abdominal infections with shock, PCT decrease to 0.5 ng/ml lacked sensitivity to predict treatment response and its decrease of at least 80% from its peak failed to accurately predict treatment response. Studies in perioperative severe infections are needed before using PCT to tailor antibiotic use in this population.
降钙素原(PCT)生物标志物被建议用于调整医学重症监护病房(ICU)的抗生素治疗,但围手术期医学方面的研究较少。本研究的目的是确定报告的PCT阈值是否与腹腔内感染继发的围手术期感染性休克的初始治疗反应相关。
这项单中心ICU观察性研究纳入了腹腔内感染继发围手术期感染性休克的患者。收集患者的人口统计学资料、第0天、第1天、第3天、第5天的PCT、治疗反应和结局。治疗失败包括与初始感染相关的死亡、二次源头控制治疗或新发腹腔内感染。主要终点是评估PCT阈值(0.5 ng/ml或从峰值下降至少80%)是否能预测初始治疗反应。
我们纳入了101例连续病例。36例患者初始治疗失败,随后的死亡率为75%。入院时,最终治疗失败的患者PCT翻倍(21.7 ng/ml±38.7 vs. 41.7 ng/ml±75.7;P = 0.04)。尽管PCT降至0.5 ng/ml以下的患者中有95%对治疗有反应,但PCT仍高于0.5 ng/ml的患者中有50%也成功对治疗有反应。此外,尽管PCT下降了至少80%,仍有40%的患者治疗失败。
在围手术期腹腔内感染伴休克的情况下,PCT降至0.5 ng/ml缺乏预测治疗反应的敏感性,且从峰值下降至少80%也未能准确预测治疗反应。在将PCT用于调整该人群的抗生素使用之前,需要开展围手术期严重感染的研究。