London School of Hygiene and Tropical Medicine, London, UK.
Eur Heart J Acute Cardiovasc Care. 2013 Sep;2(3):235-45. doi: 10.1177/2048872613487495.
It is widely thought that ST-elevation myocardial infarction (STEMI) is more likely to occur without warning (i.e. an unanticipated event in a previously healthy person) than non-ST-elevation myocardial infarction (NSTEMI), but no large study has evaluated this using prospectively collected data. The aim of this study was to compare the evolution of atherosclerotic disease and cardiovascular risk between people going on to experience STEMI and NSTEMI.
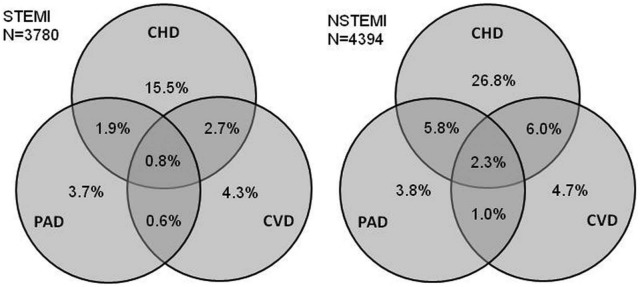
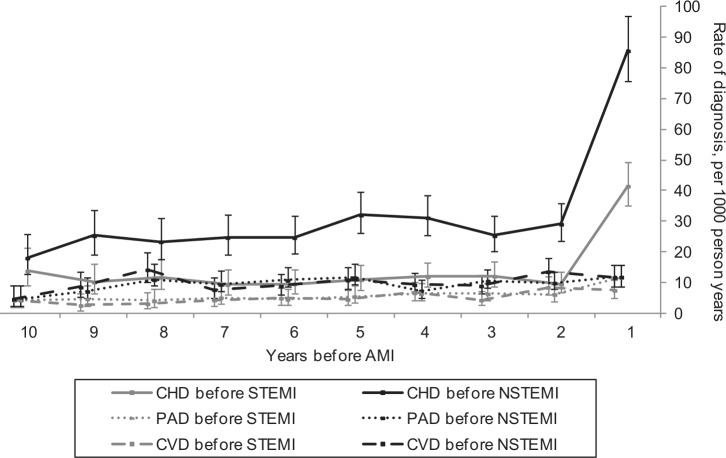
We identified patients experiencing STEMI and NSTEMI in the national registry of myocardial infarction for England and Wales (Myocardial Ischaemia National Audit Project), for whom linked primary care records were available in the General Practice Research Database (as part of the CALIBER collaboration). We compared the prevalence and timing of atherosclerotic disease and major cardiovascular risk factors including smoking, hypertension, diabetes, and dyslipidaemia, between patients later experiencing STEMI to those experiencing NSTEMI.
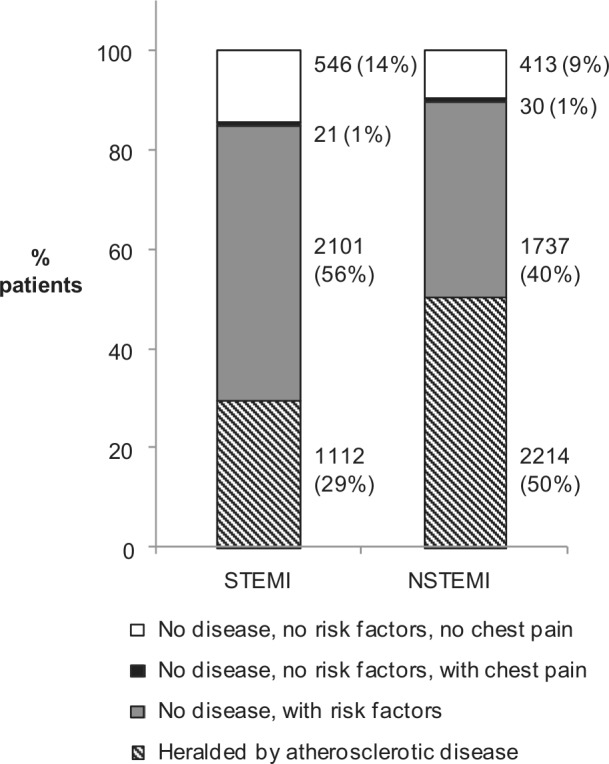
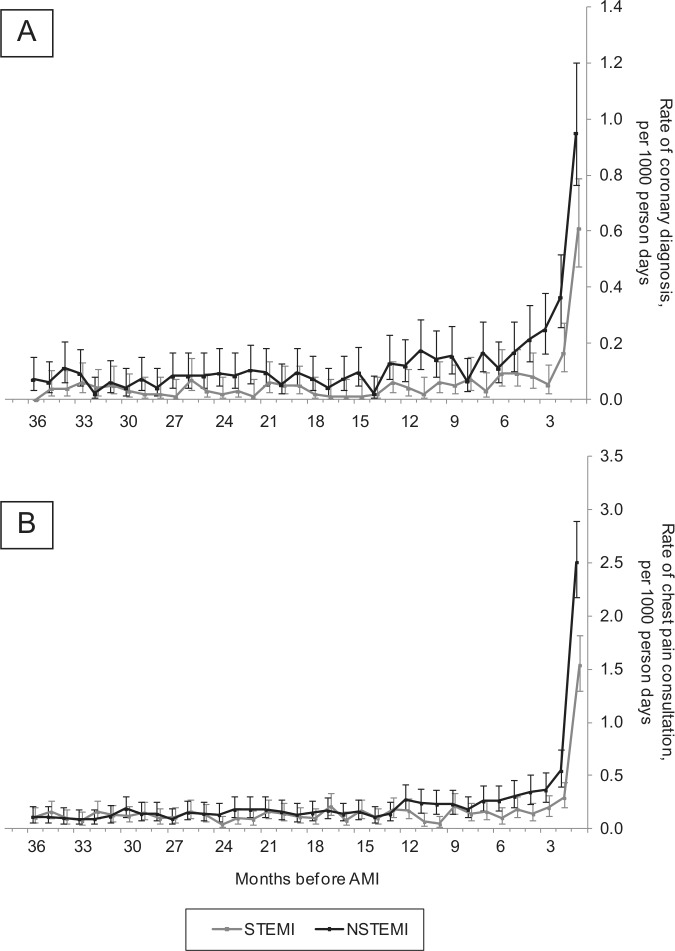
A total of 8174 myocardial infarction patients were included (3780 STEMI, 4394 NSTEMI). Myocardial infarction without heralding by previously diagnosed atherosclerotic disease occurred in 71% STEMI (95% CI 69-72%) and 50% NSTEMI patients (95% CI 48-51%). The proportions of myocardial infarctions with no prior atherosclerotic disease, major risk factors, or chest pain was 14% (95% CI 13-16%) in STEMI and 9% (95% CI 9-10%) in NSTEMI. The rate of heralding coronary diagnoses was particularly high in the 12 months before infarct; 4.1-times higher (95% CI 3.3-5.0) in STEMI and 3.6-times higher (95% CI 3.1-4.2) in NSTEMI compared to the rate in earlier years.
Acute myocardial infarction occurring without prior diagnosed coronary, cerebrovascular, or peripheral arterial disease was common, especially for STEMI. However, there was a high prevalence of risk factors or symptoms in patients without previously diagnosed disease. Better understanding of the antecedents in the year before myocardial infarction is required.
人们普遍认为 ST 段抬高型心肌梗死(STEMI)比非 ST 段抬高型心肌梗死(NSTEMI)更有可能无预警发生(即健康人群中突发的事件),但尚无大型研究使用前瞻性收集的数据对此进行评估。本研究旨在比较发生 STEMI 和 NSTEMI 的患者之间动脉粥样硬化疾病的演变和心血管风险。
我们在英格兰和威尔士的心肌梗死国家注册处(心肌缺血国家审计项目)中确定了发生 STEMI 和 NSTEMI 的患者,对于这些患者,其在全科医生研究数据库中的相关初级保健记录可作为(CALIBER 合作项目的一部分)获得。我们比较了在发生 STEMI 和 NSTEMI 后患者的动脉粥样硬化疾病和主要心血管危险因素(包括吸烟、高血压、糖尿病和血脂异常)的患病率和发生时间。
共纳入 8174 例心肌梗死患者(STEMI 3780 例,NSTEMI 4394 例)。71%(95%CI 69-72%)的 STEMI 患者和 50%(95%CI 48-51%)的 NSTEMI 患者发生了无先前诊断的动脉粥样硬化疾病的心肌梗死。无先前动脉粥样硬化疾病、主要危险因素或胸痛的心肌梗死比例在 STEMI 中为 14%(95%CI 13-16%),在 NSTEMI 中为 9%(95%CI 9-10%)。在梗死前 12 个月内,预示冠状动脉诊断的发生率特别高;STEMI 患者的发生率高出 4.1 倍(95%CI 3.3-5.0),NSTEMI 患者的发生率高出 3.6 倍(95%CI 3.1-4.2)。
无先前诊断的冠状动脉、脑血管或外周动脉疾病的急性心肌梗死很常见,尤其是 STEMI。然而,在无先前诊断疾病的患者中,危险因素或症状的患病率较高。需要更好地了解心肌梗死前一年的发病前情况。