Center for Global Health & Development, Boston University, Boston, MA, USA; Health Economics and Epidemiology Research Office, Faculty of Health Sciences, Department of Internal Medicine, School of Clinical Medicine, University of the Witwatersrand, Johannesburg, South Africa;
J Int AIDS Soc. 2013 Nov 19;16(1):18794. doi: 10.7448/IAS.16.1.18794.
In April 2010, tenofovir replaced stavudine in public-sector first-line antiretroviral therapy (ART) in South Africa. The association of tenofovir with fewer side effects and toxicities compared to stavudine could translate to increased durability of tenofovir-based regimens. We evaluated changes over time in regimen durability at the Themba Lethu Clinic, Johannesburg, South Africa.
This was a cohort analysis of treatment-naïve, non-pregnant adult patients initiated on ART between April 2004 and December 2011. First-line ART regimens before April 2010 consisted of stavudine or zidovudine with lamivudine and either efavirenz or nevirapine. Tenofovir was substituted for stavudine after April 2010. We evaluated the frequency and type of single-drug substitutions (excluding switches to second-line therapy). Cox models were used to evaluate the association of ART initiation year and antiretroviral drug type with single-drug substitutions in the first 12 months on treatment.
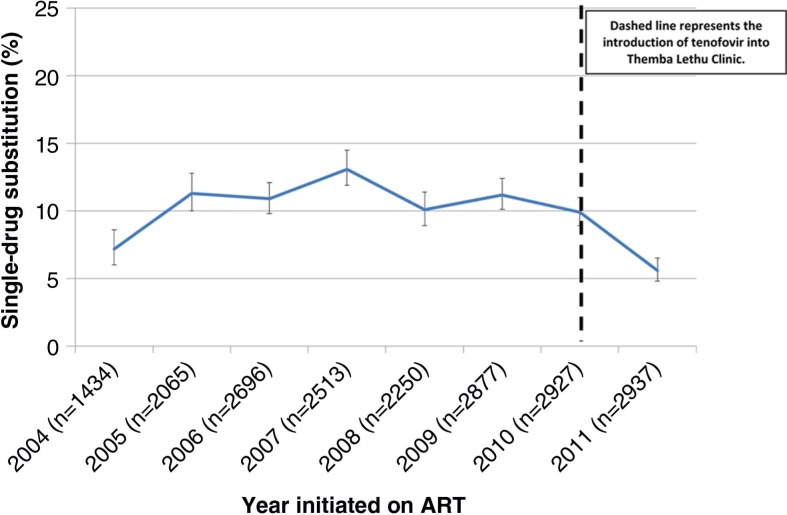
One thousand nine hundred and sixty-four (10%) substitutions occurred amongst 19,699 patients. Excluding 2004 (year of treatment roll-out), before 2010 one-year single-drug substitutions ranged from 10.0 to 13.1%. In 2011, well after integration of tenofovir, substitutions decreased to 5.6%. Single-drug substitution was lowest amongst patients on tenofovir (5.1%) versus zidovudine (11.3%), 30 mg stavudine (10.5%) or 40 mg stavudine (14.4%). Adjusted Cox models showed that patients initiating treatment between 2005 and 2010 (vs. 2011) had a twofold increased hazard of single-drug substitution, while those on zidovudine or stavudine had a two to threefold increase in single-drug substitution versus tenofovir patients in the first 12 months on ART.
The decline in single-drug substitutions is associated with the introduction of tenofovir. Tenofovir use could improve regimen durability and treatment outcomes in resource-limited settings.
2010 年 4 月,替诺福韦取代司他夫定,成为南非公共卫生部门一线抗逆转录病毒治疗(ART)的首选药物。与司他夫定相比,替诺福韦的副作用和毒性更小,这可能会使基于替诺福韦的方案更持久。我们评估了南非约翰内斯堡 Themba Lethu 诊所治疗时间的方案耐久性变化。
这是一项 2004 年 4 月至 2011 年 12 月期间开始接受 ART 的初治、非妊娠成年患者的队列分析。2010 年 4 月之前,一线 ART 方案包括司他夫定或齐多夫定,与拉米夫定联合使用,以及依非韦伦或奈韦拉平。2010 年 4 月后,替诺福韦取代了司他夫定。我们评估了治疗开始后 12 个月内单药替代(不包括二线治疗转换)的频率和类型。Cox 模型用于评估 ART 起始年份和抗逆转录病毒药物类型与治疗 12 个月内单药替代的关系。
在 19699 名患者中,有 1964 名(10%)发生了单药替代。不包括 2004 年(治疗推出的年份),2010 年之前,一年单药替代率为 10.0%至 13.1%。2011 年,在替诺福韦整合后,替代率降至 5.6%。替诺福韦组(5.1%)、齐多夫定组(11.3%)、30mg 司他夫定组(10.5%)和 40mg 司他夫定组(14.4%)的单药替代率最低。调整后的 Cox 模型显示,与 2011 年相比,2005 年至 2010 年开始治疗的患者(与 2011 年相比)单药替代的风险增加了两倍,而齐多夫定或司他夫定组与替诺福韦组相比,在 ART 治疗的前 12 个月,单药替代的风险增加了两倍至三倍。
单药替代的减少与替诺福韦的引入有关。在资源有限的环境中,替诺福韦的使用可以提高方案的耐久性和治疗效果。