Divisions of General Medicine, Massachusetts General Hospital, Boston, Massachusetts, USA.
Clin Infect Dis. 2010 Feb 1;50(3):416-25. doi: 10.1086/649884.
World Health Organization guidelines for antiretroviral treatment (ART) in resource-limited settings recommend either stavudine or tenofovir as part of initial therapy. We evaluated the clinical outcomes and cost-effectiveness of first-line ART using tenofovir in India, compared with current practice using stavudine or zidovudine.
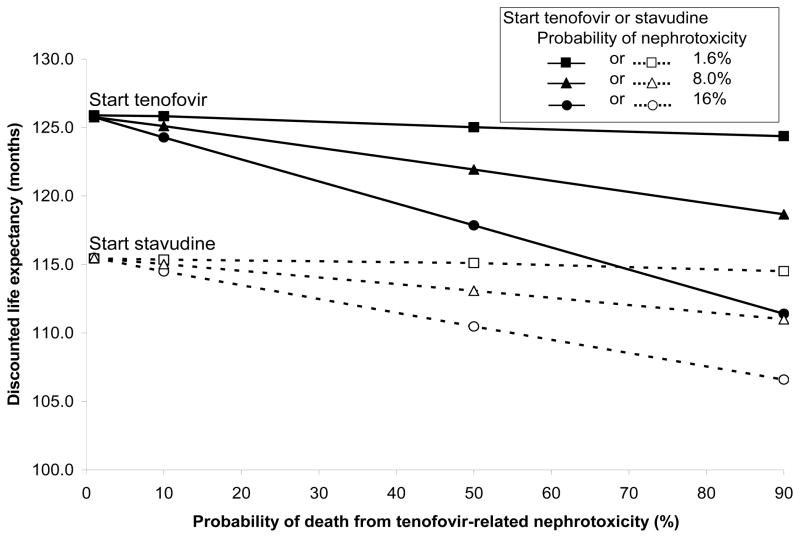
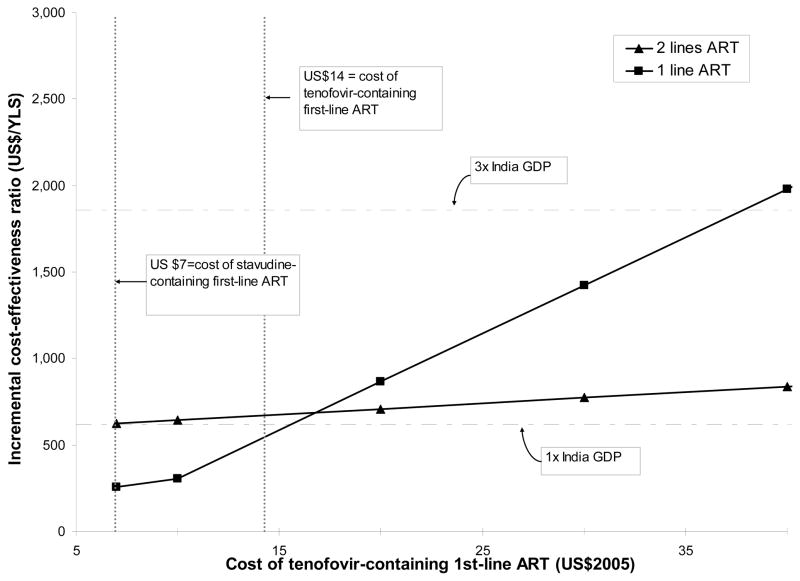
We used a state-transition model of human immunodeficiency virus (HIV) disease to examine strategies using different nucleoside reverse-transcriptase inhibitors, combined with lamivudine and nevirapine, compared with no ART: (1) stavudine, (2) stavudine with substitution by zidovudine after 6 months, (3) zidovudine, and (4) tenofovir. Data were from the Y. R. Gaitonde Centre for AIDS Research and Education in Chennai, India, and published studies. Results. Discounted mean per person survival was 36.9 months (40.2 months undiscounted) with no ART, 115.5 months (145.3) with stavudine-containing ART, 115.7 months (145.6) with stavudine and 6-month zidovudine substitution, 115.8 months (145.6) with zidovudine-containing ART, and 125.8 months (162.0) with initial tenofovir. Discounted lifetime medical costs were $610 with no ART and ranged from $5580 with stavudine-containing ART to $5720 with zidovudine-containing ART. Initial tenofovir had an incremental cost-effectiveness ratio of $670 per year of life saved, compared with no ART, and was more economically efficient than the other regimens.
were most sensitive to variations in the costs of first-line tenofovir, access to additional ART after treatment failure, and quality of life adjustment.
Using tenofovir as part of first-line ART in India will improve survival, is cost-effective by international standards, and should be considered for initial therapy for HIV-infected patients in India.
世界卫生组织在资源有限的环境下针对抗逆转录病毒治疗(ART)的指南,建议将司他夫定或替诺福韦作为初始治疗的一部分。我们评估了在印度,使用替诺福韦进行一线 ART 的临床结果和成本效益,与目前使用司他夫定或齐多夫定的情况进行了比较。
我们使用人类免疫缺陷病毒(HIV)疾病的状态转移模型,来检测使用不同核苷逆转录酶抑制剂(与拉米夫定和奈韦拉平联合使用)的策略,与不进行 ART 的策略进行比较:(1)司他夫定;(2)司他夫定在 6 个月后用齐多夫定替代;(3)齐多夫定;(4)替诺福韦。数据来自印度钦奈的 Y. R. Gaitonde 艾滋病研究和教育中心以及已发表的研究。结果:不进行 ART 的情况下,人均预期生存时间为 36.9 个月(40.2 个月未贴现),使用含司他夫定的 ART 为 115.5 个月(145.3),使用司他夫定和 6 个月齐多夫定替代为 115.7 个月(145.6),使用含齐多夫定的 ART 为 115.8 个月(145.6),而初始使用替诺福韦为 125.8 个月(162.0)。不进行 ART 的终生医疗费用为 610 美元,使用含司他夫定的 ART 的费用范围为 5580 美元至 5720 美元。与不进行 ART 相比,初始使用替诺福韦的增量成本效益比为每年每挽救 1 年生命的费用为 670 美元,且比其他方案更具有成本效益。结果对一线替诺福韦的成本、治疗失败后获得额外 ART 的机会以及生活质量调整最为敏感。结论:在印度,将替诺福韦作为一线 ART 的一部分,将提高生存率,从国际标准来看具有成本效益,并且应该考虑用于印度的 HIV 感染患者的初始治疗。