Onoya Dorina, Brennan Alana T, Berhanu Rebecca, van der Berg Liudmyla, Buthelezi Thulasizwe, Fox Matthew P
Health Economics and Epidemiology Research Office, Department of Internal Medicine, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa.
Department of Global Health, Boston University School of Public Health, Boston, MA, USA.
J Int AIDS Soc. 2016 Dec 22;19(1):20675. doi: 10.7448/IAS.19.1.20675.
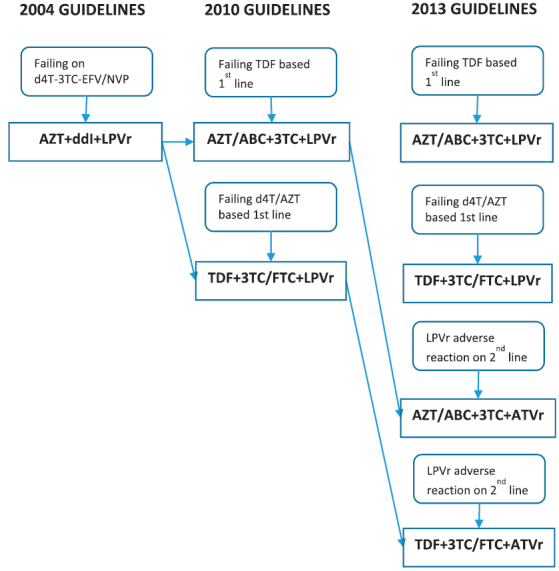
Little is known about the impact of antiretroviral therapy (ART) guideline changes on the durability of second-line ART and continuity of care. This study examines predictors of early drug substitutions and treatment interruptions using a cohort analysis of HIV positive adults switched to second-line ART between January 2004 and September 2013 in Johannesburg, South Africa.
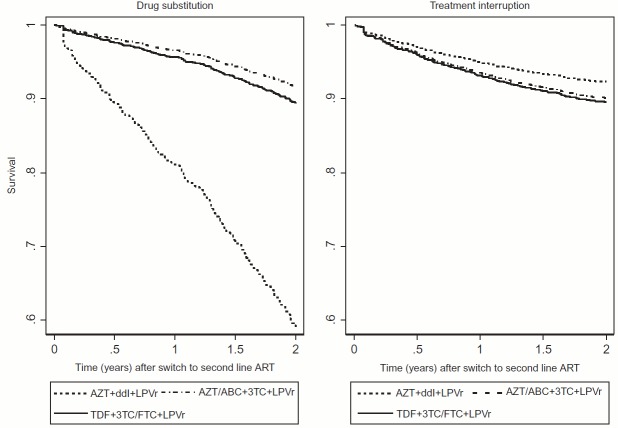
The main outcomes were having a drug substitution or treatment interruption in the first 24 months on second-line ART. Kaplan Meiers analyses and Cox proportional hazards regression were used to identify predictors of drug substitutions and treatment interruptions.
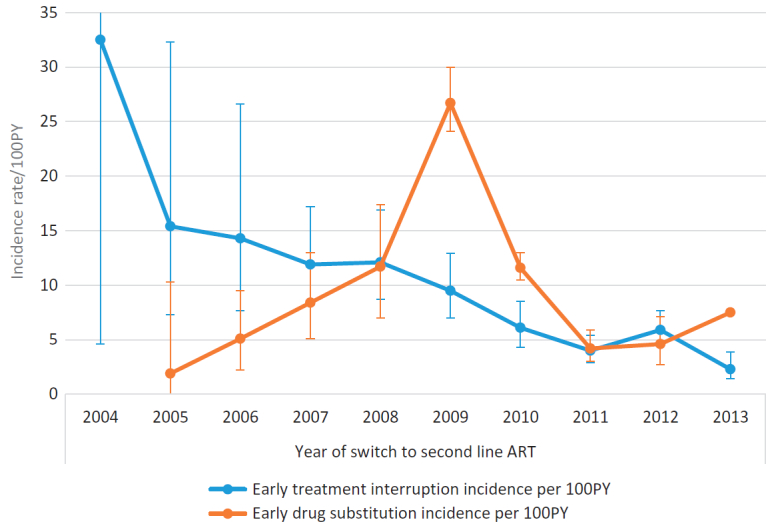
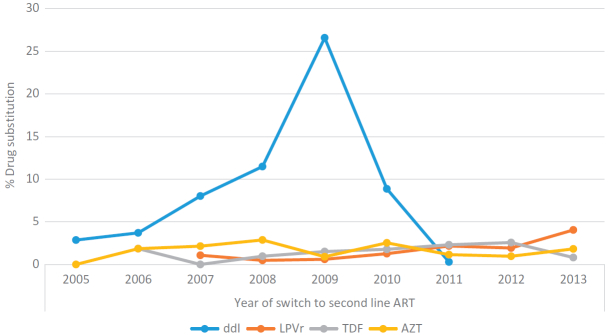
Of 3028 patients on second-line ART, 353 (11.7%) had a drug substitution (8.6 per 100PY, 95% CI: 7.8-9.6) and 260 (8.6%) had a treatment interruption (6.3 per 100PY, 95% CI: 5.6-7.1). While treatment interruptions decreased from 32.5 per 100PY for the 2004 cohort to 2.3 per 100PY for the 2013 cohort, the rates of drug substitutions steadily increased, peaking at an incidence of 26.7 per 100PY for the 2009 cohort and then decreased to 4.2 per 100PY in the 2011 cohort. Compared to the 2004 to 2008 cohorts, the hazard of early drug substitutions was highest among patients switched to AZT + ddI + LPVr in 2009 to 2010 (aHR 5.1, 95% CI: 3.4-7.1) but remained low over time among patients switched to TDF + 3TC/FTC + LPVr or AZT/ABC + 3TC + LPVr. The main common predictor of both treatment interruption and drug substitution was drug toxicity.
Our results show a rapid transition between 2004 and 2010 ART guidelines and concurrent improvements in continuity of care among second-line ART patients. Drug toxicity reporting and monitoring systems need improvements to inform timely regimen changes and ensure that patients remain in care. However, reasons for drug substitutions should be closely monitored to ensure that patients do not run out of treatment options in the future.
关于抗逆转录病毒疗法(ART)指南的变化对二线ART的持久性和护理连续性的影响,人们了解甚少。本研究通过对2004年1月至2013年9月在南非约翰内斯堡开始二线ART治疗的HIV阳性成年人进行队列分析,研究早期药物替换和治疗中断的预测因素。
主要结局是在二线ART治疗的前24个月内发生药物替换或治疗中断。采用Kaplan Meiers分析和Cox比例风险回归来确定药物替换和治疗中断的预测因素。
在3028例接受二线ART治疗的患者中,353例(11.7%)发生了药物替换(每100人年8.6例,95%可信区间:7.8-9.6),260例(8.6%)发生了治疗中断(每100人年6.3例,95%可信区间:5.6-7.1)。虽然治疗中断率从2004年队列的每100人年32.5例降至2013年队列的每100人年2.3例,但药物替换率稳步上升,在2009年队列中达到每100人年26.7例的峰值,然后在2011年队列中降至每100人年4.2例。与2004年至2008年队列相比,2009年至2010年开始使用齐多夫定+去羟肌苷+洛匹那韦/利托那韦的患者早期药物替换风险最高(调整后风险比5.1,95%可信区间:3.4-7.1),但随着时间的推移,开始使用替诺福韦+拉米夫定/恩曲他滨+洛匹那韦/利托那韦或齐多夫定/阿巴卡韦+拉米夫定+洛匹那韦/利托那韦的患者风险仍然较低。治疗中断和药物替换的主要共同预测因素是药物毒性。
我们的结果显示,2004年至2010年ART指南之间迅速转变,同时二线ART患者的护理连续性得到改善。需要改进药物毒性报告和监测系统,以便及时调整治疗方案并确保患者持续接受治疗。然而,应密切监测药物替换的原因,以确保患者未来不会用尽治疗选择。