Department of Surgery, University of Pennsylvania, Philadelphia, PA, USA,
Ann Surg Oncol. 2014 Mar;21(3):1016-23. doi: 10.1245/s10434-013-3388-5. Epub 2013 Nov 21.
Melanoma microsatellitosis is classified as stage IIIB/C disease and is associated with a poor prognosis. Prognostic factors within this group, however, have not been well characterized.
We performed a retrospective analysis of 1,621 patients undergoing sentinel lymph node (SLN) biopsy at our institution (1996-2011) to compare patients with (n = 98) and patients without (n = 1,523) microsatellites. Univariate and multivariate logistic and Cox regression analyses were used to identify factors associated with SLN positivity and melanoma-specific survival (MSS) in patients with microsatellites.
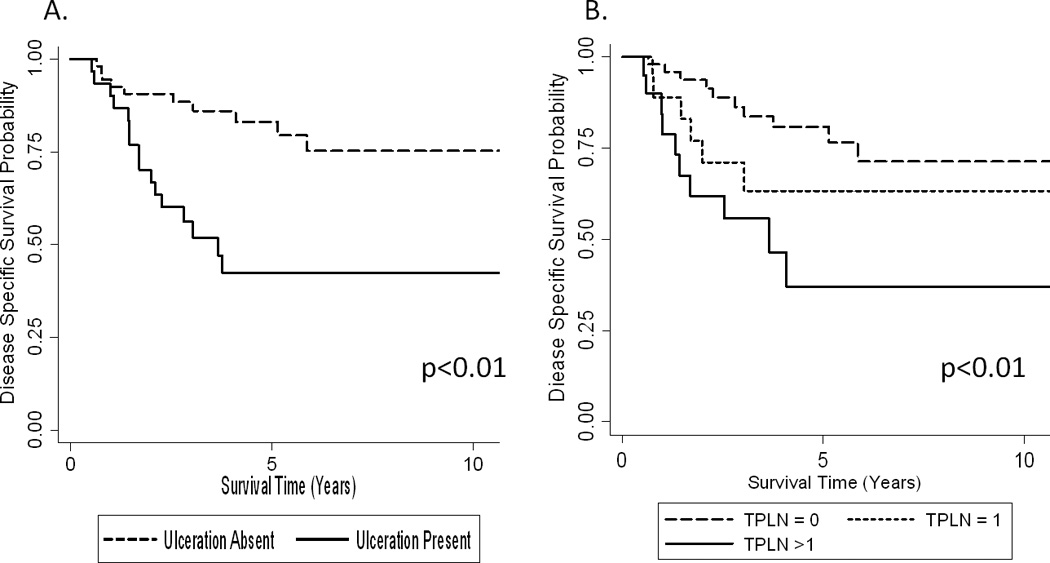
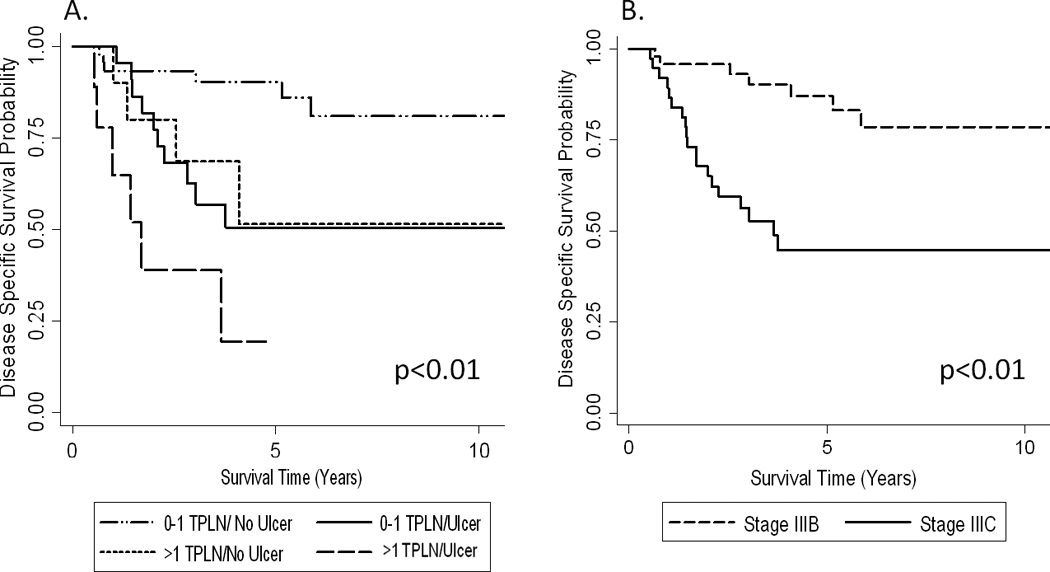
Patients with microsatellites were older and had lesions with higher Clark level and greater thickness that more frequently had mitoses, ulceration, and lymphovascular invasion (LVI) (all p < 0.0001). In microsatellite patients, the SLN positivity rate was 43 %. Lesional ulceration (odds ratio [OR] = 2.9, 95 % confidence interval [CI] 1.5-8.6), absent tumor infiltrating lymphocytes (OR = 2.8, 95 % CI 1.1-7.1), and LVI (OR = 3.3, 95 % CI 1.7-10) were significantly associated with SLN positivity by multivariate analysis. With a median follow-up of 4.5 years in survivors, ulceration (hazards ratio [HR] = 3.4, 95 % CI 1.5-7.8) and >1 metastatic LN (HR = 2.7, 95 % CI 1.1-6.6) were significantly associated with decreased MSS by multivariate analysis. In patients without these prognostic factors, the 5-year MSS was 90 % (n = 49) compared with 50 % (n = 23) among patients with ulceration only, 51 % (n = 12) in those with >1 metastatic LN only, or 25 % in those with both (n = 14, p < 0.01).
Microsatellitosis was frequently associated with multiple adverse pathologic features. In the absence of ulceration and >1 metastatic LN; however, the outcome for patients with microsatellites compared favorably to stage IIIB patients overall.
黑色素瘤微卫星不稳定性被归类为 IIIB/C 期疾病,与预后不良相关。然而,该亚组内的预后因素尚未得到很好的描述。
我们对在我院接受前哨淋巴结 (SLN) 活检的 1621 例患者(1996-2011 年)进行了回顾性分析,以比较有(n=98)和无(n=1523)微卫星的患者。采用单变量和多变量逻辑和 Cox 回归分析来确定与微卫星患者的 SLN 阳性和黑色素瘤特异性生存 (MSS) 相关的因素。
有微卫星的患者年龄较大,病变的 Clark 级别和厚度更高,更常出现有丝分裂、溃疡和淋巴管血管侵犯 (LVI)(均 p<0.0001)。在微卫星患者中,SLN 阳性率为 43%。病变溃疡(优势比 [OR] = 2.9,95%置信区间 [CI] 1.5-8.6)、缺乏肿瘤浸润淋巴细胞(OR = 2.8,95%CI 1.1-7.1)和 LVI(OR = 3.3,95%CI 1.7-10)在多变量分析中与 SLN 阳性显著相关。在幸存者的中位随访 4.5 年后,溃疡(风险比 [HR] = 3.4,95%CI 1.5-7.8)和 >1 个转移淋巴结(HR = 2.7,95%CI 1.1-6.6)在多变量分析中与 MSS 降低显著相关。在没有这些预后因素的患者中,5 年 MSS 为 90%(n=49),而仅有溃疡的患者为 50%(n=23),仅有 >1 个转移淋巴结的患者为 51%(n=12),两者均有的患者为 25%(n=14,p<0.01)。
黑色素瘤微卫星不稳定性常与多种不良病理特征相关。然而,在没有溃疡和 >1 个转移淋巴结的情况下,与总体 IIIB 期患者相比,有微卫星的患者的结局较好。