Herzig K-H, Ahola R, Leppäluoto J, Jokelainen J, Jämsä T, Keinänen-Kiukaanniemi S
1] Institute of Biomedicine, Department of Physiology and Biocenter of Oulu, Oulu University, Oulu, Finland [2] Medical Research Center Oulu and Oulu University Hospital, Oulu, Finland.
Department of Medical Technology, University of Oulu, Oulu, Finland.
Int J Obes (Lond). 2014 Aug;38(8):1089-96. doi: 10.1038/ijo.2013.224. Epub 2013 Nov 28.
To examine physical activity (PA) thresholds affecting glucose, insulin and lipid concentrations and body fat composition in high-risk patients for type 2 diabetes (T2D).
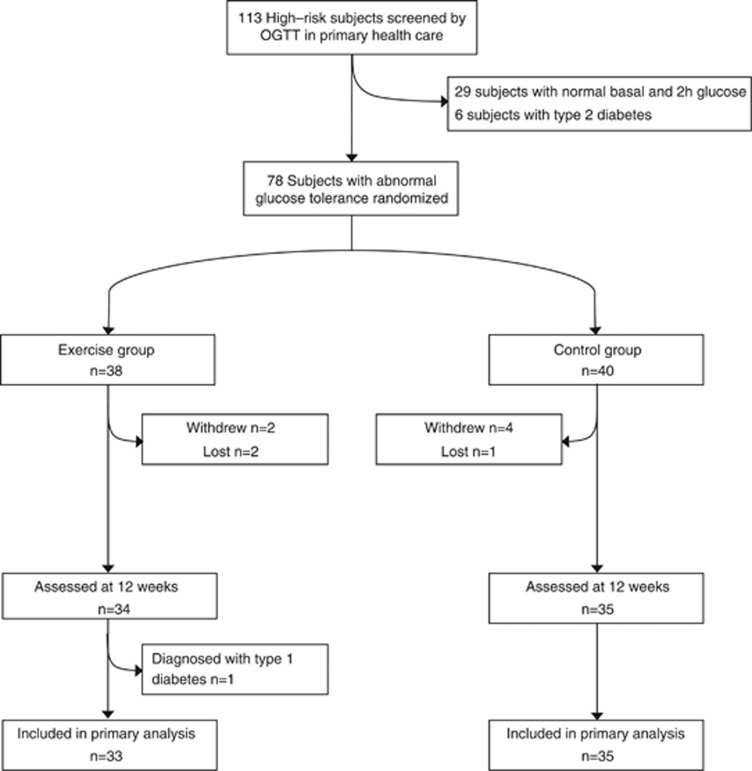
A total of 113 subjects of both genders having abnormal glucose levels in the oral glucose tolerance test were contacted. A total of 78 subjects with age 58.8±10.4 years and body mass index 31.7±5.3 kg m(-2) were randomly assigned to intervention and control groups. INTERVENTION consisted of a supervised walking (60 min three times weekly) for 3 months. All the subjects received standard care for PA and weight reduction and wore an accelerometer during the whole wakeful time.
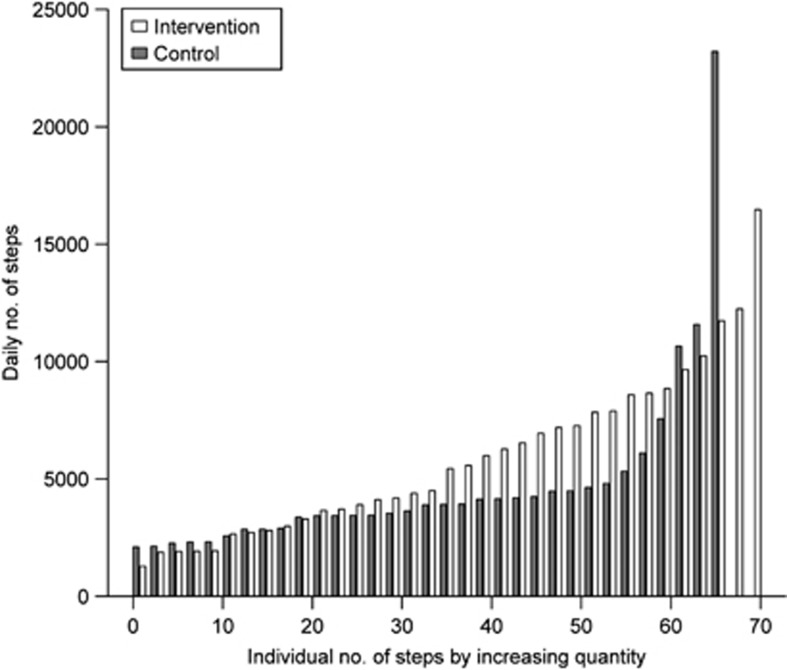
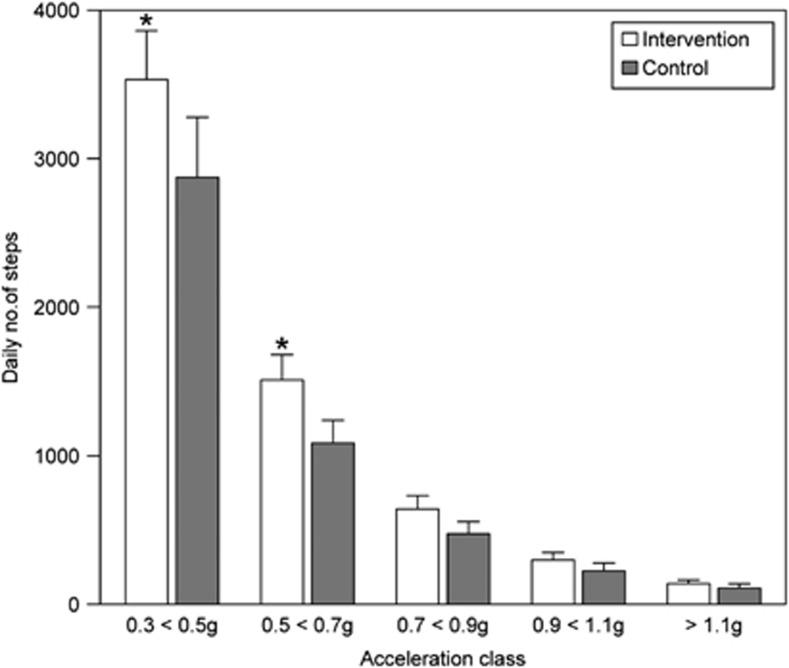
Over 80% of the daily steps clustered at an acceleration level of 0.3-0.7 g (2-3 km h(-1) of walking) and were 5870 in the intervention and 4434 in the control group (P<0.029). Between 0 and 3 months no significant changes were observed in fasting and 2-h glucose, body weight or maximal oxygen uptake. In contrast, changes in fasting and 2-h insulin (-3.4 mU l(-1), P=0.035 and -26.6, P=0.003, respectively), homeostasis model assessment-estimated insulin resistance (-1.0, P=0.036), total cholesterol (-0.55 mmol l(-1), P=0.041), low-density lipoprotein (LDL) cholesterol (-0.36 mmol l(-1), P=0.008) and visceral fat area (-5.5 cm(2), P=0.030) were significantly greater in the intervention than in control subjects. The overall effects of PA were analyzed by quartiles of daily steps of all subjects. There were significant reductions in total and LDL cholesterol and visceral fat area between the highest (daily steps over 6520) and the lowest quartile (1780-2810 daily steps). The changes associated with PA remained significant after adjustments of baseline, sex, age and body weight change.
Habitual and structured PAs with the acceleration levels of 0.3-0.7 g and daily steps over 6520, equivalent to walking at 2-3 km h(-1) for 90 min daily, standing for the relative PA intensity of 30-35% of the maximal oxygen uptake, are clinically beneficial for overweight/obese and physically inactive individuals with a high risk for T2D.
研究影响2型糖尿病(T2D)高危患者血糖、胰岛素、血脂浓度及体脂成分的身体活动(PA)阈值。
联系了113名在口服葡萄糖耐量试验中血糖水平异常的男女受试者。将78名年龄为58.8±10.4岁、体重指数为31.7±5.3kg/m²的受试者随机分为干预组和对照组。干预措施包括在监督下每周步行3次、每次60分钟,持续3个月。所有受试者均接受关于PA和减重的标准护理,并在整个清醒时间佩戴加速度计。
超过80%的每日步数集中在0.3 - 0.7g的加速度水平(相当于步行速度2 - 3km/h),干预组为5870步,对照组为4434步(P<0.029)。在0至3个月期间,空腹和餐后2小时血糖、体重或最大摄氧量未观察到显著变化。相比之下,干预组空腹和餐后2小时胰岛素(分别为-3.4mU/l,P = 0.035;-26.6,P = 0.003)、稳态模型评估估算的胰岛素抵抗(-1.0,P = 0.036)、总胆固醇(-0.55mmol/l,P = 0.041)、低密度脂蛋白(LDL)胆固醇(-0.36mmol/l,P = 0.008)和内脏脂肪面积(-5.5cm²,P = 0.030)的变化显著大于对照组。通过所有受试者每日步数的四分位数分析PA的总体效果。最高四分位数组(每日步数超过6520步)与最低四分位数组(每日步数1780 - 2810步)相比,总胆固醇、LDL胆固醇和内脏脂肪面积显著降低。在调整基线、性别、年龄和体重变化后,与PA相关的变化仍然显著。
对于超重/肥胖且身体活动不足的T2D高危个体,习惯性且结构化的PA,加速度水平为0.3 - 0.7g且每日步数超过6520步,相当于每天以2 - 3km/h的速度步行90分钟,代表最大摄氧量的30 - 35%的相对PA强度,在临床上是有益的。