Carpeggiani Clara, Marraccini Paolo, Morales Maria Aurora, Prediletto Renato, Landi Patrizia, Picano Eugenio
CNR, Institute of Clinical Physiology, Pisa, Italy.
PLoS One. 2013 Nov 27;8(11):e81161. doi: 10.1371/journal.pone.0081161. eCollection 2013.
Radiological inappropriateness in medical imaging leads to loss of resources and accumulation of avoidable population cancer risk. Aim of the study was to audit the appropriateness rate of different cardiac radiological examinations.
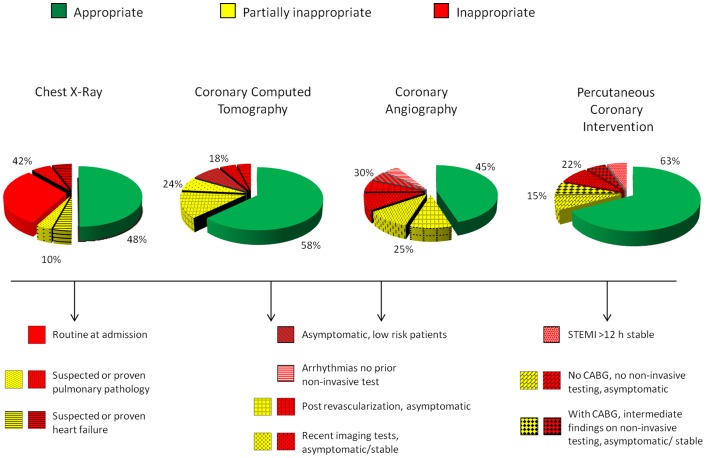
With a retrospective, observational study we reviewed clinical records of 818 consecutive patients (67 ± 12 years, 75% males) admitted from January 1-May 31, 2010 to the National Research Council - Tuscany Region Gabriele Monasterio Foundation cardiology division. A total of 940 procedures were audited: 250 chest x-rays (CXR); 240 coronary computed tomographies (CCT); 250 coronary angiographies (CA); 200 percutaneous coronary interventions (PCI). For each test, indications were rated on the basis of guidelines class of recommendation and level of evidence: definitely appropriate (A, including class I, appropriate, and class IIa, probably appropriate), uncertain (U, class IIb, probably inappropriate), or inappropriate (I, class III, definitely inappropriate). Appropriateness was suboptimal for all tests: CXR (A = 48%, U = 10%, I = 42%); CCT (A = 58%, U = 24%, I = 18%); CA (A = 45%, U = 25%, I = 30%); PCI (A = 63%, U = 15%, I = 22%). Top reasons for inappropriateness were: routine on hospital admission (70% of inappropriate CXR); first line application in asymptomatic low-risk patients (42% of CCT) or in patients with unchanged clinical status post-revascularization (20% of CA); PCI in patients either asymptomatic or with miscellaneous symptoms and without inducible ischemia on non-invasive testing (36% of inappropriate PCI).
Public healthcare system--with universal access paid for with public money--is haemorrhaging significant resources and accumulating avoidable long-term cancer risk with inappropriate cardiovascular imaging prevention.
医学影像中的放射学不恰当性会导致资源浪费以及可避免的人群癌症风险累积。本研究的目的是审核不同心脏放射学检查的恰当率。
通过一项回顾性观察研究,我们回顾了2010年1月1日至5月31日期间连续收治到国家研究委员会 - 托斯卡纳地区加布里埃莱·莫纳斯特里奥基金会心脏病科的818例患者(67±12岁,75%为男性)的临床记录。共审核了940项检查:250例胸部X光(CXR);240例冠状动脉计算机断层扫描(CCT);250例冠状动脉造影(CA);200例经皮冠状动脉介入治疗(PCI)。对于每项检查,根据指南推荐类别和证据水平对适应证进行评级:肯定恰当(A,包括I类,恰当,以及IIa类,可能恰当)、不确定(U,IIb类,可能不恰当)或不恰当(I,III类,肯定不恰当)。所有检查的恰当性均未达到最佳:CXR(A = 48%,U = 10%,I = 42%);CCT(A = 58%,U = 24%,I = 18%);CA(A = 45%,U = 25%,I = 30%);PCI(A = 63%,U = 15%,I = 22%)。不恰当的主要原因包括:入院常规检查(70%的不恰当CXR);在无症状低风险患者中作为一线检查(42%的CCT)或在血管重建术后临床状态未改变的患者中进行(20%的CA);在无症状或有多种症状且无创检查无诱发缺血的患者中进行PCI(36%的不恰当PCI)。
由公共资金支付、全民可及的公共医疗系统正因不恰当的心血管影像检查而大量流失资源,并累积可避免的长期癌症风险。