Vasaturo Angela, Di Blasio Stefania, Peeters Deborah G A, de Koning Coco C H, de Vries Jolanda M, Figdor Carl G, Hato Stanleyson V
Department of Tumor Immunology, Nijmegen Centre for Molecular Life Sciences, Radboud University Nijmegen Medical Centre , Nijmegen , Netherlands.
Department of Tumor Immunology, Nijmegen Centre for Molecular Life Sciences, Radboud University Nijmegen Medical Centre , Nijmegen , Netherlands ; Department of Medical Oncology, Nijmegen Centre for Molecular Life Sciences, Radboud University Nijmegen Medical Centre , Nijmegen , Netherlands.
Front Immunol. 2013 Dec 3;4:417. doi: 10.3389/fimmu.2013.00417.
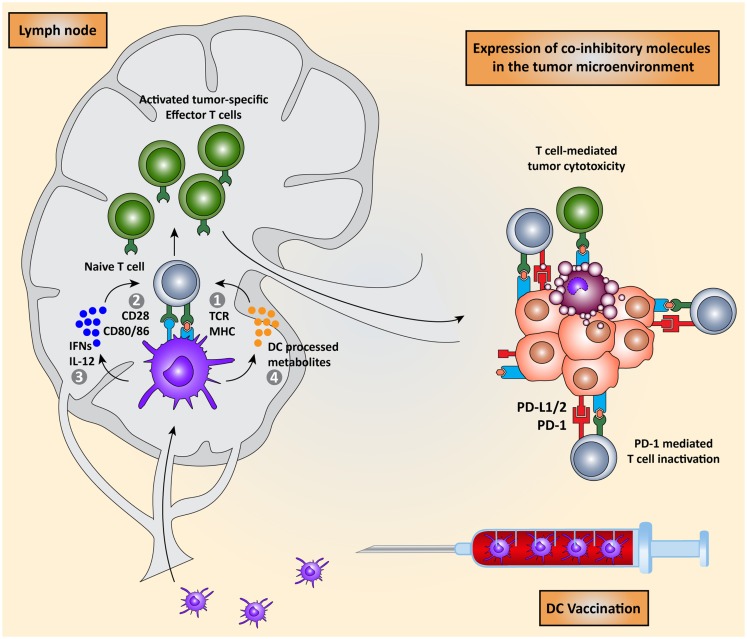
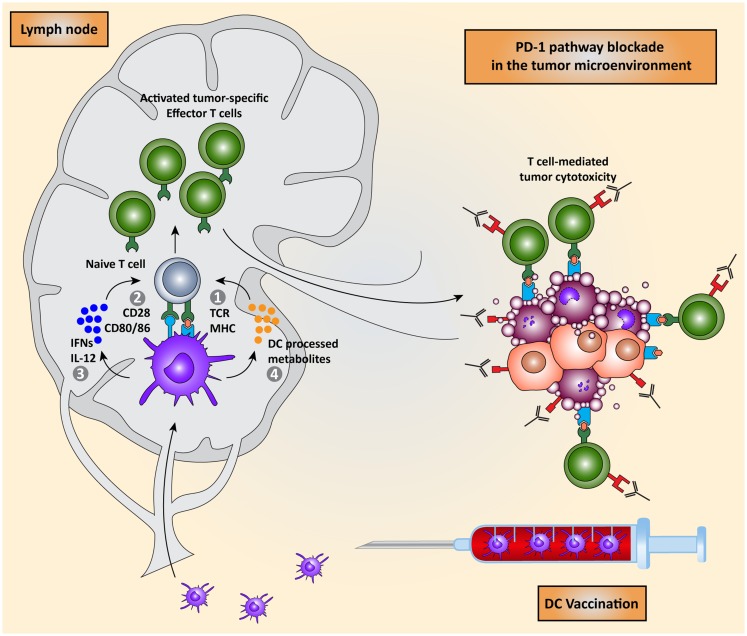
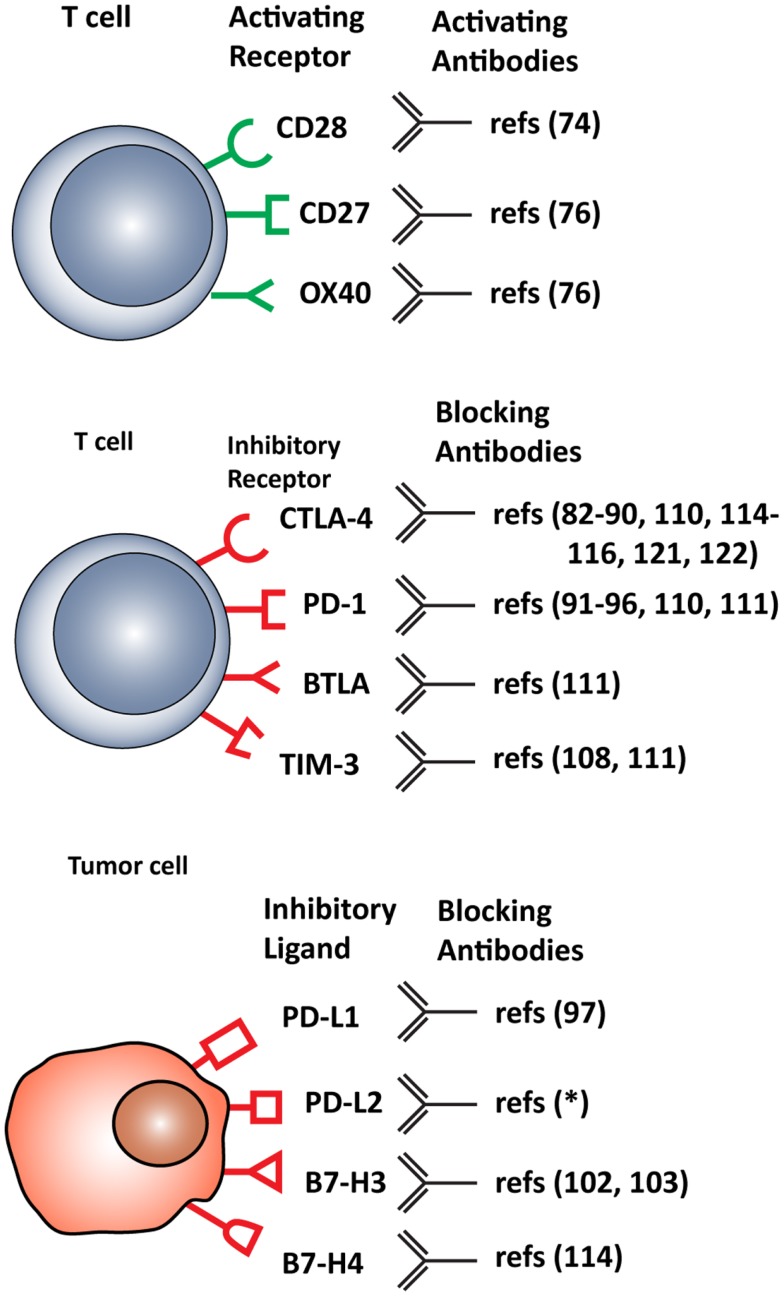
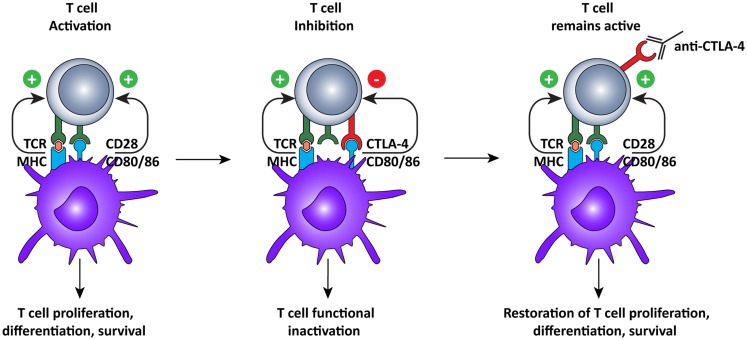
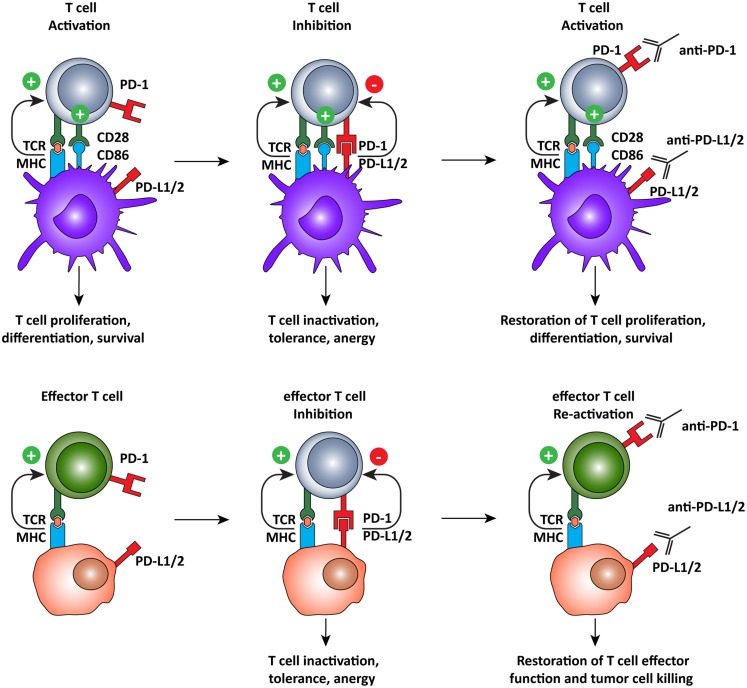
The aim of therapeutic dendritic cell (DC) vaccines in cancer immunotherapy is to activate cytotoxic T cells to recognize and attack the tumor. T cell activation requires the interaction of the T cell receptor with a cognate major-histocompatibility complex-peptide complex. Although initiated by antigen engagement, it is the complex balance between co-stimulatory and co-inhibitory signals on DCs that results in T cell activation or tolerance. Even when already activated, tumor-specific T cells can be neutralized by the expression of co-inhibitory molecules on tumor cells. These and other immunosuppressive cues in the tumor microenvironment are major factors currently hampering the application of DC vaccination. In this review, we discuss recent data regarding the essential and complex role of co-inhibitory molecules in regulating the immune response within the tumor microenvironment. In particular, possible therapeutic intervention strategies aimed at reversing or neutralizing suppressive networks within the tumor microenvironment will be emphasized. Importantly, blocking co-inhibitory molecule signaling, often referred to as immune checkpoint blockade, does not necessarily lead to an effective activation of tumor-specific T cells. Therefore, combination of checkpoint blockade with other immune potentiating therapeutic strategies, such as DC vaccination, might serve as a synergistic combination, capable of reversing effector T cells immunosuppression while at the same time increasing the efficacy of T cell-mediated immunotherapies. This will ultimately result in long-term anti-tumor immunity.
治疗性树突状细胞(DC)疫苗在癌症免疫治疗中的目的是激活细胞毒性T细胞以识别并攻击肿瘤。T细胞的激活需要T细胞受体与同源的主要组织相容性复合体-肽复合物相互作用。尽管由抗原结合引发,但DC上共刺激信号和共抑制信号之间的复杂平衡才导致T细胞的激活或耐受。即使已经被激活,肿瘤特异性T细胞也可被肿瘤细胞上共抑制分子的表达所中和。肿瘤微环境中的这些以及其他免疫抑制因素是目前阻碍DC疫苗应用的主要因素。在本综述中,我们讨论了关于共抑制分子在调节肿瘤微环境内免疫反应中重要且复杂作用的最新数据。特别强调了旨在逆转或中和肿瘤微环境内抑制网络的可能治疗干预策略。重要的是,阻断共抑制分子信号传导,通常称为免疫检查点阻断,不一定会导致肿瘤特异性T细胞的有效激活。因此,检查点阻断与其他免疫增强治疗策略(如DC疫苗接种)的联合应用可能是一种协同组合,能够逆转效应T细胞的免疫抑制,同时提高T细胞介导的免疫治疗效果。这最终将产生长期的抗肿瘤免疫力。