Ozkan Burak, Güngör Durmus, Yıldırım Utku Mahir, Harman Ali, Ozen Ozgur, Aytekin Cüneyt
Department of Interventional Radiology, Baskent University School Of Medicine, Ankara, Turkey.
Iran J Radiol. 2013 Sep;10(3):133-9. doi: 10.5812/iranjradiol.11386. Epub 2013 Aug 30.
In hemodialysis patients, the most common problem in arteriovenous fistulas, as the best functional vascular access, is the juxtaanastomotic located lesions. Percutaneous transluminal angioplasty is accepted as the treatment method for juxtanastomotic lesions.
To assess juxtaanastomotic stent placement after insufficient balloon angioplasty in the treatment of autogenous radiocephalic or brachiocephalic fistula dysfunction.
Between July 2003 and June 2010, 20 hemodialysis patients with autogenous radiocephalic or brachiocephalic fistula dysfunction underwent stent placement for the lesion located at the juxtaanastomotic region. Indications for stent placement were insufficient balloon dilatation, early recurring stenosis, chronic organizing thrombus and vessel rupture. The Kaplan-Meier method was used to calculate the stent patency rates. All patients who had fistula dysfunction (thrombosis of hemodialysis access, difficult access cannulation, extremity pain due to thrombosis or decreased arterial access blood flow) were evaluated by color Doppler ultrasound. The stenoses were initially dilated with standard noncompliant balloons (3 to 10-mm in diameter). Dilatation was followed by high pressure (Blue Max, Boston Scientific) or cutting balloons (Boston Scientific), if the standard balloon failed to dilate the stenotic segment.
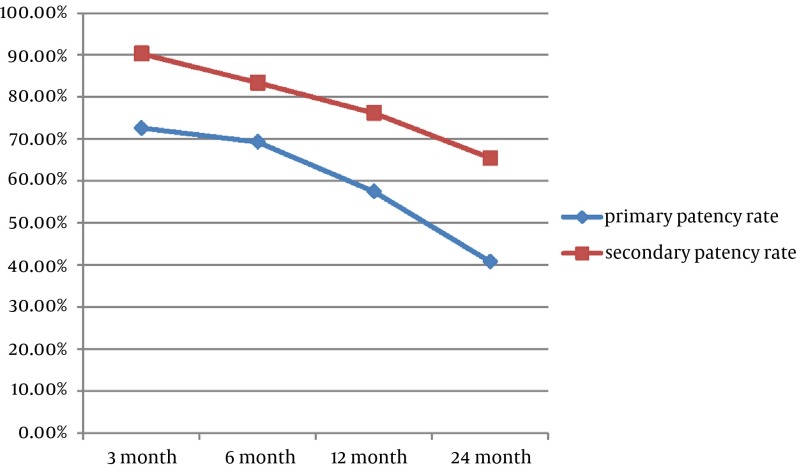
Twenty-one stents were applied. The anatomical and clinical success rate was 100%. Seventeen additional interventions were done for 11 (55%) patients due to stent thrombosis or stenosis during follow-up. Our 1- and 2-year secondary patency rates were 76.2% and 65.5%, respectively and were comparable to those after balloon angioplasty and surgical shunt revision.
Metallic stent placement is a safe and effective procedure for salvage of native hemodialysis fistula after unsuccessful balloon angioplasty.
在血液透析患者中,作为最佳功能性血管通路的动静脉内瘘最常见的问题是吻合口附近病变。经皮腔内血管成形术被公认为是治疗吻合口附近病变的方法。
评估在球囊血管成形术效果不佳后,置入吻合口附近支架治疗自体桡动脉头静脉或肱动脉头静脉内瘘功能障碍的效果。
2003年7月至2010年6月期间,20例患有自体桡动脉头静脉或肱动脉头静脉内瘘功能障碍的血液透析患者因吻合口附近区域病变接受了支架置入术。置入支架的指征为球囊扩张不足、早期复发性狭窄、慢性机化血栓和血管破裂。采用Kaplan-Meier法计算支架通畅率。所有有内瘘功能障碍(血液透析通路血栓形成、穿刺困难、因血栓形成导致肢体疼痛或动脉通路血流减少)的患者均接受彩色多普勒超声评估。狭窄最初用标准的非顺应性球囊(直径3至10毫米)扩张。如果标准球囊未能扩张狭窄段,则在扩张后使用高压球囊(Blue Max,波士顿科学公司)或切割球囊(波士顿科学公司)。
共置入21枚支架。解剖学和临床成功率为100%。随访期间,11例(55%)患者因支架血栓形成或狭窄又进行了17次干预。我们的1年和2年二次通畅率分别为76.2%和65.5%,与球囊血管成形术和手术分流修复后的通畅率相当。
在球囊血管成形术失败后,置入金属支架是挽救自体血液透析内瘘的一种安全有效的方法。