Centre for Medical Imaging, University College London, London, United Kingdom.
Department of Primary Care Health Sciences, University of Oxford, Oxford, United Kingdom.
PLoS One. 2013 Dec 9;8(12):e80767. doi: 10.1371/journal.pone.0080767. eCollection 2013.
To establish the relative weighting given by patients and healthcare professionals to gains in diagnostic sensitivity versus loss of specificity when using CT colonography (CTC) for colorectal cancer screening.
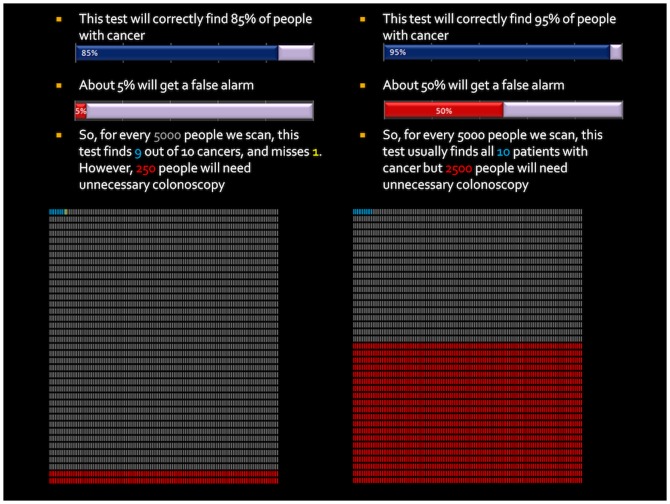
Following ethical approval and informed consent, 75 patients and 50 healthcare professionals undertook a discrete choice experiment in which they chose between "standard" CTC and "enhanced" CTC that raised diagnostic sensitivity 10% for either cancer or polyps in exchange for varying levels of specificity. We established the relative increase in false-positive diagnoses participants traded for an increase in true-positive diagnoses.
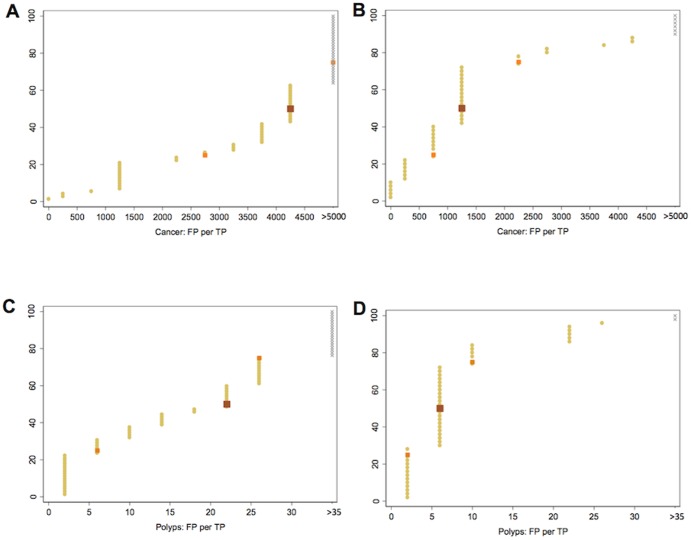
Data from 122 participants were analysed. There were 30 (25%) non-traders for the cancer scenario and 20 (16%) for the polyp scenario. For cancer, the 10% gain in sensitivity was traded up to a median 45% (IQR 25 to >85) drop in specificity, equating to 2250 (IQR 1250 to >4250) additional false-positives per additional true-positive cancer, at 0.2% prevalence. For polyps, the figure was 15% (IQR 7.5 to 55), equating to 6 (IQR 3 to 22) additional false-positives per additional true-positive polyp, at 25% prevalence. Tipping points were significantly higher for patients than professionals for both cancer (85 vs 25, p<0.001) and polyps (55 vs 15, p<0.001). Patients were willing to pay significantly more for increased sensitivity for cancer (p = 0.021).
When screening for colorectal cancer, patients and professionals believe gains in true-positive diagnoses are worth much more than the negative consequences of a corresponding rise in false-positives. Evaluation of screening tests should account for this.
确定在使用 CT 结肠成像(CTC)进行结直肠癌筛查时,患者和医疗保健专业人员对诊断敏感度提高与特异性损失的相对权重,当涉及 CTC 用于结直肠癌筛查时,患者和医疗保健专业人员在诊断敏感度提高与特异性损失之间进行权衡。
在获得伦理批准和知情同意后,75 名患者和 50 名医疗保健专业人员参与了一项离散选择实验,他们在“标准”CTC 和“增强”CTC 之间进行选择,“增强”CTC 可将癌症或息肉的诊断敏感度提高 10%,但特异性会相应降低。我们确定了参与者为提高真阳性诊断而愿意交换的假阳性诊断的相对增加量。
对 122 名参与者的数据进行了分析。在癌症情况下,有 30 名(25%)参与者是非交易者,在息肉情况下,有 20 名(16%)参与者是非交易者。对于癌症,10%的敏感度增益最多可换取 45%(IQR 25%至>85%)的特异性下降,相当于每增加一个真阳性癌症,就会增加 2250 个(IQR 1250 至>4250 个)额外的假阳性诊断,在 0.2%的患病率下。对于息肉,这一数字为 15%(IQR 7.5%至 55%),相当于每增加一个真阳性息肉,就会增加 6 个(IQR 3 至 22 个)额外的假阳性诊断,在 25%的患病率下。对于癌症和息肉,患者的转折点均显著高于专业人员(癌症:85 比 25,p<0.001;息肉:55 比 15,p<0.001)。患者对癌症的敏感度提高愿意支付的费用明显更高(p=0.021)。
在结直肠癌筛查中,患者和专业人员认为真阳性诊断的收益远高于假阳性诊断增加的负面后果。因此,筛查试验的评估应该考虑到这一点。