Warren Alpert Medical School, Brown University, Providence, Rhode Island, United States of America.
Department of Community Health, Rwanda Ministry of Health, Kigali, Kigali Province, Rwanda.
PLoS One. 2013 Dec 3;8(12):e82386. doi: 10.1371/journal.pone.0082386. eCollection 2013.
To investigate the accuracy of three clinical scales for predicting severe disease (severe dehydration or death) in children with diarrhea in a resource-limited setting.
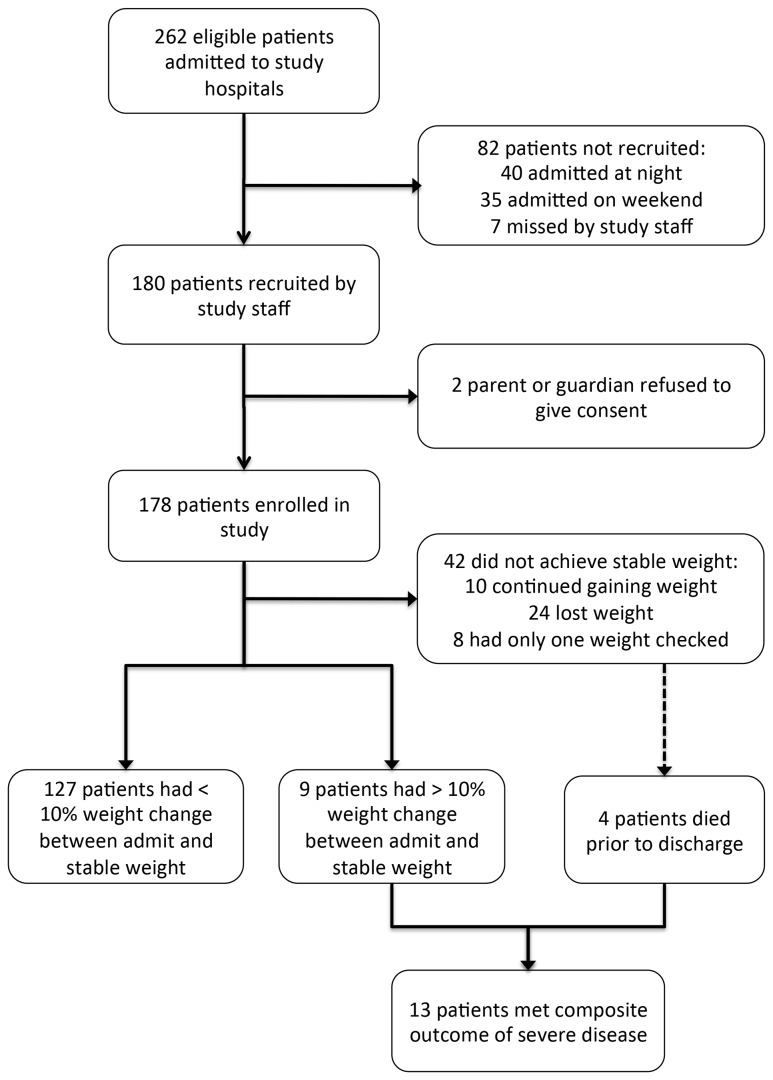
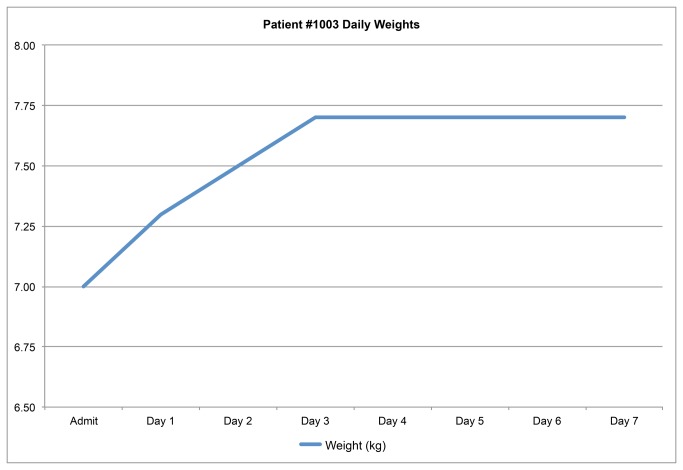
Participants included 178 children admitted to three Rwandan hospitals with diarrhea. A local physician or nurse assessed each child on arrival using the World Health Organization (WHO) severe dehydration scale and the Centers for Disease Control (CDC) scale. Children were weighed on arrival and daily until they achieved a stable weight, with a 10% increase between admission weight and stable weight considered severe dehydration. The Clinical Dehydration Scale was then constructed post-hoc using the data collected for the other two scales. Receiver Operator Characteristic (ROC) curves were constructed for each scale compared to the composite outcome of severe dehydration or death.
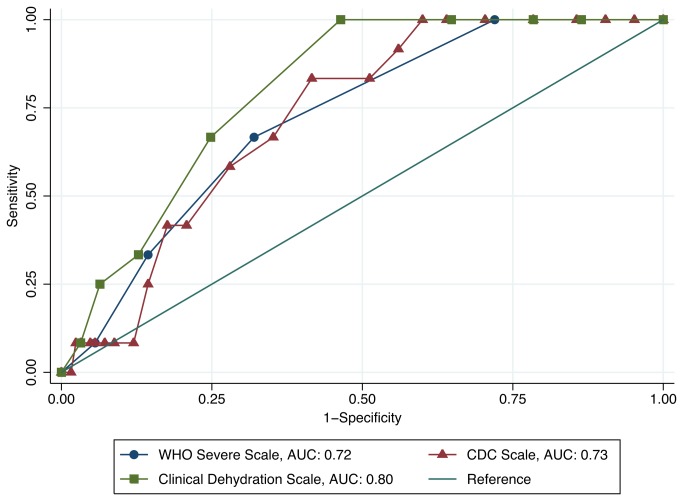
The WHO severe dehydration scale, CDC scale, and Clinical Dehydration Scale had areas under the ROC curves (AUCs) of 0.72 (95% CI 0.60, 0.85), 0.73 (95% CI 0.62, 0.84), and 0.80 (95% CI 0.71, 0.89), respectively, in the full cohort. Only the Clinical Dehydration Scale was a significant predictor of severe disease when used in infants, with an AUC of 0.77 (95% CI 0.61, 0.93), and when used by nurses, with an AUC of 0.78 (95% CI 0.63, 0.93).
While all three scales were moderate predictors of severe disease in children with diarrhea, scale accuracy varied based on provider training and age of the child. Future research should focus on developing or validating clinical tools that can be used accurately by nurses and other less-skilled providers to assess all children with diarrhea in resource-limited settings.
在资源有限的环境下,研究三种临床量表在预测腹泻儿童严重疾病(严重脱水或死亡)方面的准确性。
共有 178 名在卢旺达三家医院就诊的腹泻儿童参与本研究。当地医生或护士在抵达时分别使用世界卫生组织(WHO)严重脱水量表和美国疾病控制与预防中心(CDC)量表对每个儿童进行评估。在抵达时以及每日对儿童进行称重,直到他们达到稳定体重,入院体重与稳定体重之间的 10%增长被认为是严重脱水。然后,根据另外两种量表收集的数据,构建临床脱水量表。构建每个量表与严重脱水或死亡复合结局的受试者工作特征(ROC)曲线。
WHO 严重脱水量表、CDC 量表和临床脱水量表的 ROC 曲线下面积(AUC)分别为 0.72(95%CI 0.60,0.85)、0.73(95%CI 0.62,0.84)和 0.80(95%CI 0.71,0.89)。只有临床脱水量表在婴儿中是严重疾病的显著预测因子,AUC 为 0.77(95%CI 0.61,0.93),在护士中使用时,AUC 为 0.78(95%CI 0.63,0.93)。
虽然这三种量表都是儿童腹泻严重疾病的中度预测因子,但根据提供者的培训和儿童的年龄,量表的准确性有所不同。未来的研究应集中于开发或验证临床工具,以便在资源有限的环境中由护士和其他技能较低的提供者准确使用,评估所有腹泻儿童。