The Warren Alpert Medical School of Brown University, Providence, RI, USA
The Warren Alpert Medical School of Brown University, Providence, RI, USA.
Glob Health Sci Pract. 2015 Aug 18;3(3):405-18. doi: 10.9745/GHSP-D-15-00097.
Diarrhea remains one of the most common and most deadly conditions affecting children worldwide. Accurately assessing dehydration status is critical to determining treatment course, yet no clinical diagnostic models for dehydration have been empirically derived and validated for use in resource-limited settings.
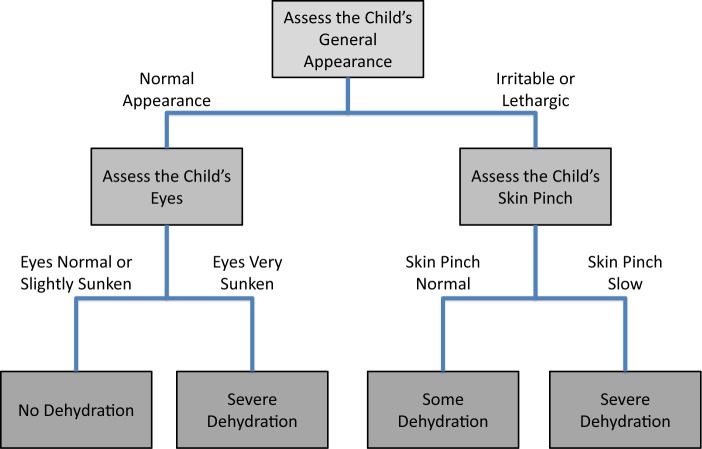
In the Dehydration: Assessing Kids Accurately (DHAKA) prospective cohort study, a random sample of children under 5 with acute diarrhea was enrolled between February and June 2014 in Bangladesh. Local nurses assessed children for clinical signs of dehydration on arrival, and then serial weights were obtained as subjects were rehydrated. For each child, the percent weight change with rehydration was used to classify subjects with severe dehydration (>9% weight change), some dehydration (3-9%), or no dehydration (<3%). Clinical variables were then entered into logistic regression and recursive partitioning models to develop the DHAKA Dehydration Score and DHAKA Dehydration Tree, respectively. Models were assessed for their accuracy using the area under their receiver operating characteristic curve (AUC) and for their reliability through repeat clinical exams. Bootstrapping was used to internally validate the models.
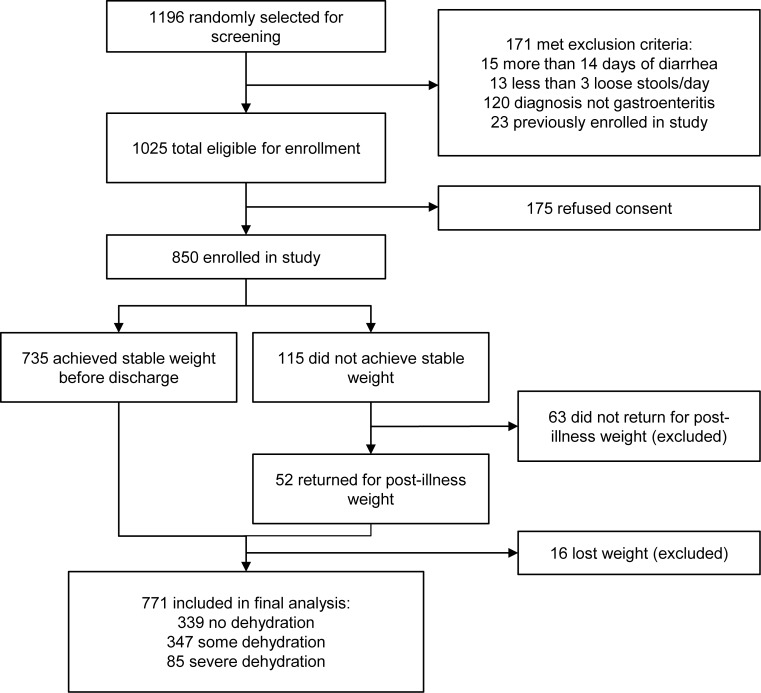
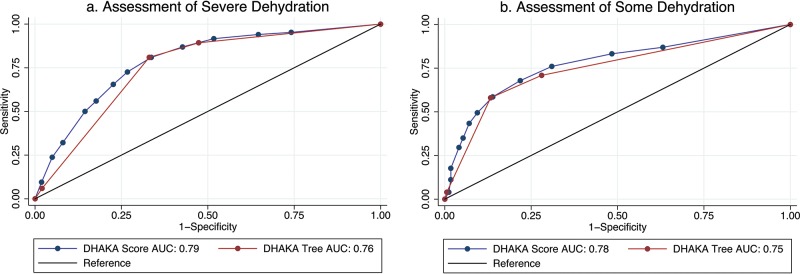
A total of 850 children were enrolled, with 771 included in the final analysis. Of the 771 children included in the analysis, 11% were classified with severe dehydration, 45% with some dehydration, and 44% with no dehydration. Both the DHAKA Dehydration Score and DHAKA Dehydration Tree had significant AUCs of 0.79 (95% CI = 0.74, 0.84) and 0.76 (95% CI = 0.71, 0.80), respectively, for the diagnosis of severe dehydration. Additionally, the DHAKA Dehydration Score and DHAKA Dehydration Tree had significant positive likelihood ratios of 2.0 (95% CI = 1.8, 2.3) and 2.5 (95% CI = 2.1, 2.8), respectively, and significant negative likelihood ratios of 0.23 (95% CI = 0.13, 0.40) and 0.28 (95% CI = 0.18, 0.44), respectively, for the diagnosis of severe dehydration. Both models demonstrated 90% agreement between independent raters and good reproducibility using bootstrapping.
This study is the first to empirically derive and internally validate accurate and reliable clinical diagnostic models for dehydration in a resource-limited setting. After external validation, frontline providers may use these new tools to better manage acute diarrhea in children.
腹泻仍然是全球范围内最常见和最致命的儿童疾病之一。准确评估脱水状态对于确定治疗方案至关重要,但在资源有限的环境中,尚未有经验性推导和验证的脱水临床诊断模型。
在腹泻:准确评估儿童(DHAKA)前瞻性队列研究中,2014 年 2 月至 6 月期间在孟加拉国招募了年龄在 5 岁以下、患有急性腹泻的随机样本儿童。当地护士在儿童到达时评估其脱水的临床体征,然后在儿童接受补液时获得连续体重。对于每个儿童,用补液后体重变化的百分比来分类,其中严重脱水(体重变化>9%)、有些脱水(3-9%)或无脱水(<3%)。然后将临床变量输入逻辑回归和递归分区模型,分别开发 DHAKA 脱水评分和 DHAKA 脱水树。使用接收器操作特征曲线(AUC)下面积评估模型的准确性,并通过重复临床检查评估模型的可靠性。使用自举法对内部分别对模型进行验证。
共纳入 850 名儿童,其中 771 名纳入最终分析。在纳入分析的 771 名儿童中,11%被诊断为严重脱水,45%为有些脱水,44%为无脱水。DHAKA 脱水评分和 DHAKA 脱水树对严重脱水的诊断均具有显著的 AUC,分别为 0.79(95%CI=0.74, 0.84)和 0.76(95%CI=0.71, 0.80)。此外,DHAKA 脱水评分和 DHAKA 脱水树对严重脱水的阳性似然比分别为 2.0(95%CI=1.8, 2.3)和 2.5(95%CI=2.1, 2.8),阴性似然比分别为 0.23(95%CI=0.13, 0.40)和 0.28(95%CI=0.18, 0.44)。两个模型在独立评估者之间具有 90%的一致性,并且使用自举法具有良好的可重复性。
本研究首次在资源有限的环境中经验性推导和内部验证了用于脱水的准确可靠的临床诊断模型。经过外部验证,一线医护人员可能会使用这些新工具来更好地管理儿童急性腹泻。