Jauregui Joshua, Nelson Daniel, Choo Esther, Stearns Branden, Levine Adam C, Liebmann Otto, Shah Sachita P
Warren Alpert Medical School Department of Emergency Medicine, Brown University, Providence, Rhode Island, United States of America; Division of Emergency Medicine, University of Washington, Seattle, Washington, United States of America.
Warren Alpert Medical School Department of Emergency Medicine, Brown University, Providence, Rhode Island, United States of America.
PLoS One. 2014 May 2;9(5):e95739. doi: 10.1371/journal.pone.0095739. eCollection 2014.
To prospectively validate three popular clinical dehydration scales and overall physician gestalt in children with vomiting or diarrhea relative to the criterion standard of percent weight change with rehydration.
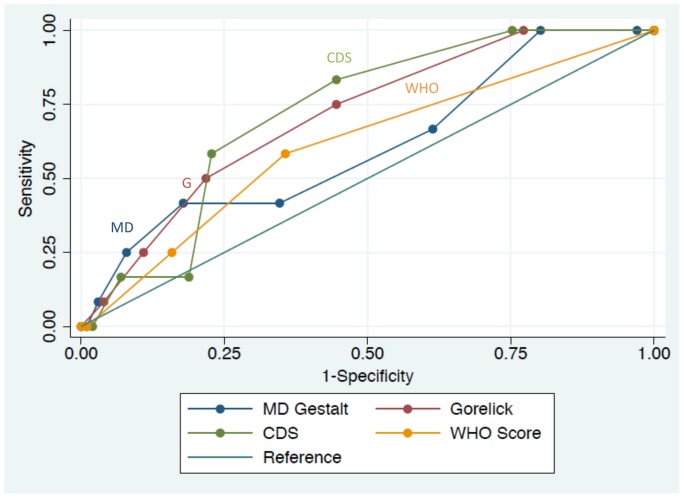
We prospectively enrolled a non-consecutive cohort of children ≤ 18 years of age with an acute episode of diarrhea or vomiting. Patient weight, clinical scale variables and physician clinical impression, or gestalt, were recorded before and after fluid resuscitation in the emergency department and upon hospital discharge. The percent weight change from presentation to discharge was used to calculate the degree of dehydration, with a weight change of ≥ 5% considered significant dehydration. Receiver operating characteristics (ROC) curves were constructed for each of the three clinical scales and physician gestalt. Sensitivity and specificity were calculated based on the best cut-points of the ROC curve.
We approached 209 patients, and of those, 148 were enrolled and 113 patients had complete data for analysis. Of these, 10.6% had significant dehydration based on our criterion standard. The Clinical Dehydration Scale (CDS) and Gorelick scales both had an area under the ROC curve (AUC) statistically different from the reference line with AUCs of 0.72 (95% CI 0.60, 0.84) and 0.71 (95% CI 0.57, 0.85) respectively. The World Health Organization (WHO) scale and physician gestalt had AUCs of 0.61 (95% CI 0.45, 0.77) and 0.61 (0.44, 0.78) respectively, which were not statistically significant.
The Gorelick scale and Clinical Dehydration Scale were fair predictors of dehydration in children with diarrhea or vomiting. The World Health Organization scale and physician gestalt were not helpful predictors of dehydration in our cohort.
相对于补液后体重变化百分比这一标准,前瞻性验证三种常用的儿童呕吐或腹泻临床脱水量表以及医生整体判断的准确性。
我们前瞻性纳入了一组年龄≤18岁、患有急性腹泻或呕吐发作的非连续队列儿童。在急诊科进行液体复苏前、后以及出院时记录患者体重、临床量表变量和医生的临床印象(即整体判断)。从就诊到出院的体重变化百分比用于计算脱水程度,体重变化≥5%被视为严重脱水。为三种临床量表和医生整体判断分别构建受试者工作特征(ROC)曲线。根据ROC曲线的最佳切点计算敏感性和特异性。
我们接触了209名患者,其中148名被纳入研究,113名患者有完整数据可供分析。在这些患者中,根据我们的标准,10.6%患有严重脱水。临床脱水量表(CDS)和戈列里克量表的ROC曲线下面积(AUC)与参考线相比均有统计学差异,AUC分别为0.72(95%CI 0.60, 0.84)和0.71(95%CI 0.57, 0.85)。世界卫生组织(WHO)量表和医生整体判断的AUC分别为0.61(95%CI 0.45, 0.77)和0.61(0.44, 0.78),无统计学意义。
戈列里克量表和临床脱水量表是腹泻或呕吐儿童脱水的较好预测指标。在我们的队列中,世界卫生组织量表和医生整体判断对脱水的预测作用不大。