Mohan Sumit, Huff Edwin, Wish Jay, Lilly Michael, Chen Shu-Cheng, McClellan William M
Division of Nephrology, Department of Medicine, Columbia University College of Physicians & Surgeons, New York, New York, United States of America.
Division of Quality Improvement, Centers for Medicare & Medicaid Services, Boston Regional Office, Boston, Massachusetts, United States of America.
PLoS One. 2013 Dec 17;8(12):e83447. doi: 10.1371/journal.pone.0083447. eCollection 2013.
Patients started on long term hemodialysis have typically had low rates of reported renal recovery with recent estimates ranging from 0.9-2.4% while higher rates of recovery have been reported in cohorts with higher percentages of patients with acute renal failure requiring dialysis.
Our analysis followed approximately 194,000 patients who were initiated on hemodialysis during a 2-year period (2008 & 2009) with CMS-2728 forms submitted to CMS by dialysis facilities, cross-referenced with patient record updates through the end of 2010, and tracked through December 2010 in the CMS SIMS registry.
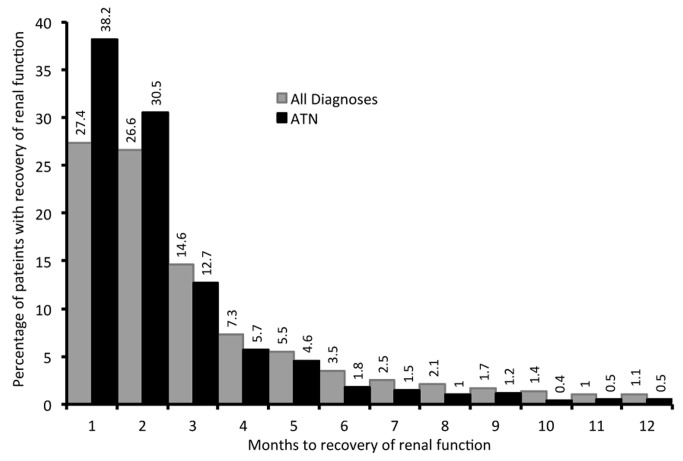
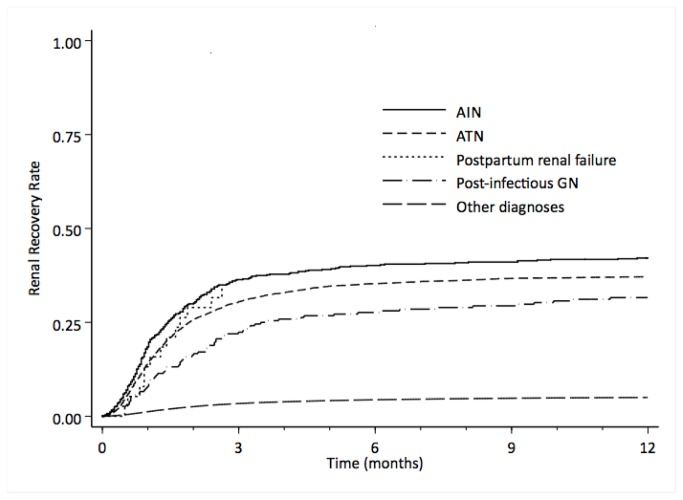
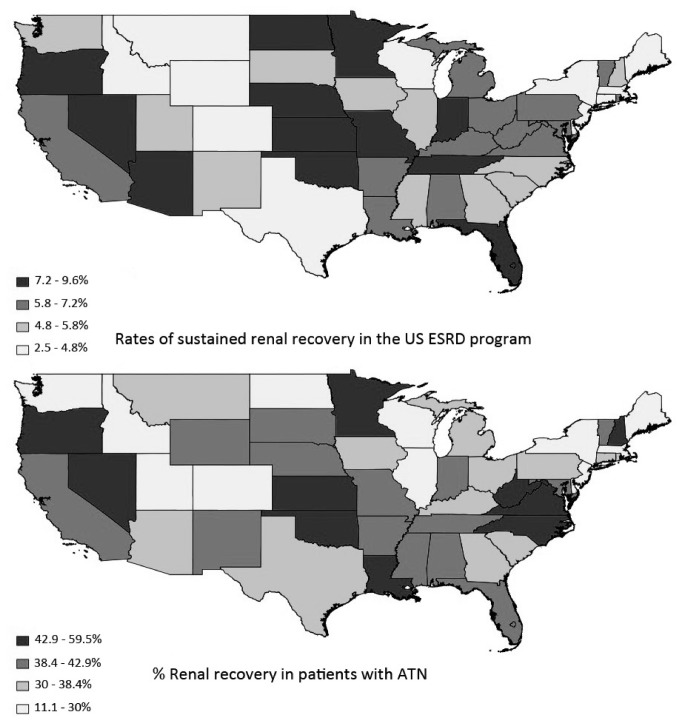
We report a sustained renal recovery (i.e no return to ESRD during the available follow up period) rate among Medicare ESRD patients of > 5% - much higher than previously reported. Recovery occurred primarily in the first 2 months post incident dialysis, and was more likely in cases with renal failure secondary to etiologies associated with acute kidney injury. Patients experiencing sustained recovery were markedly less likely than true long-term ESRD patients to have permanent vascular accesses in place at incident hemodialysis, while non-White patients, and patients with any prior nephrology care appeared to have significantly lower rates of renal recovery. We also found widespread geographic variation in the rates of renal recovery across the United States.
Renal recovery rates in the US Medicare ESRD program are higher than previously reported and appear to have significant geographic variation. Patients with diagnoses associated with acute kidney injury who are initiated on long-term hemodialysis have significantly higher rates of renal recovery than the general ESRD population and lower rates of permanent access placement.
开始接受长期血液透析的患者,其报告的肾脏恢复率通常较低,最近的估计范围为0.9%-2.4%,而在因急性肾衰竭需要透析的患者比例较高的队列中,报告的恢复率较高。
我们的分析跟踪了约194,000名在2年期间(2008年和2009年)开始接受血液透析的患者,透析机构向医疗保险和医疗补助服务中心(CMS)提交了CMS-2728表格,并与截至2010年底的患者记录更新进行交叉参考,并在CMS SIMS登记处跟踪至2010年12月。
我们报告医疗保险终末期肾病(ESRD)患者的持续肾脏恢复率(即在可用的随访期内未恢复到ESRD)>5%,远高于先前报告的水平。恢复主要发生在首次透析后的前2个月,并且在继发于与急性肾损伤相关病因的肾衰竭病例中更有可能发生。与真正的长期ESRD患者相比,经历持续恢复的患者在首次血液透析时进行永久性血管通路的可能性明显更低,而非白人患者以及任何先前接受过肾病护理的患者的肾脏恢复率似乎明显更低。我们还发现美国各地肾脏恢复率存在广泛的地理差异。
美国医疗保险ESRD项目中的肾脏恢复率高于先前报告的水平,并且似乎存在显著的地理差异。因急性肾损伤相关诊断而开始接受长期血液透析的患者,其肾脏恢复率明显高于一般ESRD人群,且永久性通路置入率较低。