Department of Gynecologic Oncology, Chaim Sheba Medical Center, Ramat Gan, 5262000, Israel.
1] Sunnybrook Health Sciences Center, Toronto, Ontario, Canada M4N 3M5 [2] Department of Gynecologic Oncology, University of Toronto, 27 King's College Circle, Toronto, Ontario, Canada M5S 1A1.
Br J Cancer. 2014 Feb 4;110(3):609-15. doi: 10.1038/bjc.2013.766. Epub 2013 Dec 24.
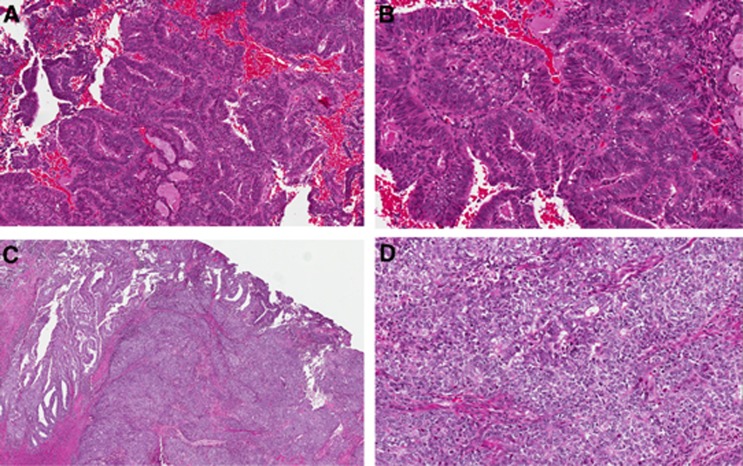
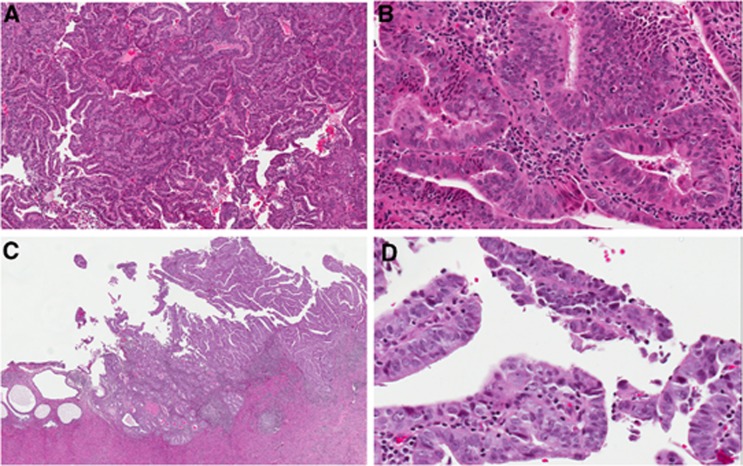
The histology and grade of endometrial cancer are important predictors of disease outcome and of the likelihood of nodal involvement. In most centres, however, surgical staging decisions are based on a preoperative biopsy. The objective of this study was to assess the concordance between the preoperative histology and that of the hysterectomy specimen in endometrial cancer.
Patients treated for endometrial cancer during a 10-year period at a tertiary cancer centre were identified from a prospectively collected pathological database. All pathology reports were reviewed to confirm centralised reporting of the original sampling or biopsy specimens; patients whose biopsies were not reviewed by a dedicated gynaecological pathologist at the treating centre were excluded. Surgical pathology data including histology, grade, depth of myometrial invasion, cervical stromal involvement and lymphovascular space invasion (LVSI) as well as preoperative histology and grade were collected. Preoperative and final tumour cell type and grade were compared and the distribution of other high-risk features was analysed.
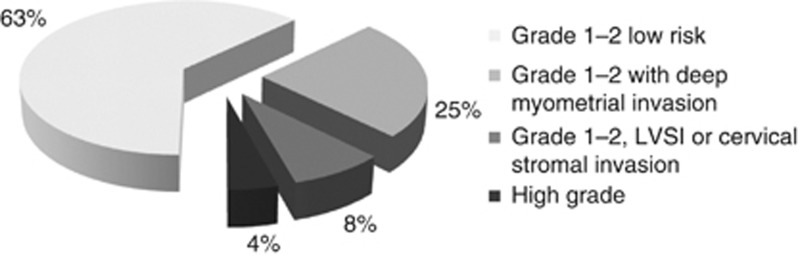
A total of 1329 consecutive patients were identified; 653 patients had a centrally reviewed epithelial endometrial cancer on their original biopsy, and are included in this study. Of 255 patients whose biopsies were read as grade 1 (G1) adenocarcinoma, 45 (18%) were upgraded to grade 2 (G2) on final pathology, 6 (2%) were upgraded to grade 3 (G3) and 5 (2%) were read as a non-endometrioid high-grade histology. Overall, of 255 tumours classified as G1 endometrioid cancers on biopsy, 74 (29%) were either found to be low-grade (G1-2) tumours with deep myometrial invasion, or were reclassified as high-grade cancers (G3 or non-endometrioid histologies) on final surgical pathology. Despite these shifts, we calculate that omitting surgical staging in preoperatively diagnosed G1 endometrioid cancers without deep myometrial invasion would result in missing nodal involvement in only 1% of cases.
Preoperative endometrial sampling is only a modest predictor of surgical pathology features in endometrial cancer and may underestimate the risk of disease spread and recurrence. In spite of frequent shifts in postoperative vs preoperative histological assessment, the predicted rate of missed nodal metastases with a selective staging policy remains low.
子宫内膜癌的组织学和分级是疾病结局和淋巴结受累可能性的重要预测因素。然而,在大多数中心,手术分期决策是基于术前活检。本研究的目的是评估子宫内膜癌术前组织学与子宫切除术标本之间的一致性。
从一家三级癌症中心前瞻性收集的病理数据库中确定了在 10 年内接受子宫内膜癌治疗的患者。所有病理报告均经过审查,以确认原始采样或活检标本的中心化报告;在治疗中心未由专门的妇科病理学家审查活检的患者被排除在外。收集了手术病理数据,包括组织学、分级、肌层浸润深度、宫颈基质受累和脉管间隙浸润(LVSI)以及术前组织学和分级。比较了术前和最终肿瘤细胞类型和分级,并分析了其他高危特征的分布。
共确定了 1329 例连续患者;653 例患者的原始活检有中央审查的上皮性子宫内膜癌,包括在本研究中。在 255 例活检分级为 1 级(G1)腺癌的患者中,45 例(18%)在最终病理中升级为 2 级(G2),6 例(2%)升级为 3 级(G3),5 例(2%)被归类为非子宫内膜样高级别组织学。总体而言,在 255 例活检分级为 G1 子宫内膜样癌的肿瘤中,74 例(29%)要么发现为深部肌层浸润的低级别(G1-2)肿瘤,要么在最终手术病理中重新分类为高级别癌症(G3 或非子宫内膜样组织学)。尽管存在这些变化,但我们计算出,如果在术前诊断为 G1 子宫内膜样癌且无深部肌层浸润的患者中省略手术分期,仅会导致 1%的病例漏诊淋巴结受累。
术前子宫内膜取样只是子宫内膜癌手术病理特征的适度预测指标,可能低估疾病扩散和复发的风险。尽管术后与术前组织学评估存在频繁变化,但采用选择性分期策略,预测漏诊淋巴结转移的发生率仍然较低。