1Division of Oncology, The Children's Hospital of Philadelphia, Philadelphia, PA. 2Department of Pediatrics, University of Pennsylvania Perelman School of Medicine, Philadelphia, PA. 3Department of Anesthesia and Critical Care Medicine, The Children's Hospital of Philadelphia, Philadelphia, PA. 4Center for Clinical Epidemiology and Biostatistics, University of Pennsylvania Perelman School of Medicine, Philadelphia, PA. 5Division of Infectious Diseases, The Children's Hospital of Philadelphia, Philadelphia, PA. 6Center for Pediatric Clinical Effectiveness, The Children's Hospital of Philadelphia, Philadelphia, PA. 7Bristol-Myers Squibb, Hopewell, NJ. 8Division of Haematology/Oncology and Program in Child Health Evaluative Sciences, The Hospital for Sick Children, Toronto, ON, Canada. 9Department of Biostatistics and Epidemiology, University of Pennsylvania Perelman School of Medicine, Philadelphia, PA. 10Division of Pediatric Critical Care Medicine, Department of Pediatrics and Public Health Sciences, Penn State Hershey Milton S. Hershey Medical Center, Hershey, PA.
Pediatr Crit Care Med. 2014 Feb;15(2):112-20. doi: 10.1097/PCC.0000000000000042.
Children with acute myeloid leukemia are at risk for sepsis and organ failure. Outcomes associated with intensive care support have not been studied in a large pediatric acute myeloid leukemia population. Our objective was to determine hospital mortality of pediatric acute myeloid leukemia patients requiring intensive care.
Retrospective cohort study of children hospitalized between 1999 and 2010. Use of intensive care was defined by utilization of specific procedures and resources. The primary endpoint was hospital mortality.
Forty-three children's hospitals contributing data to the Pediatric Health Information System database.
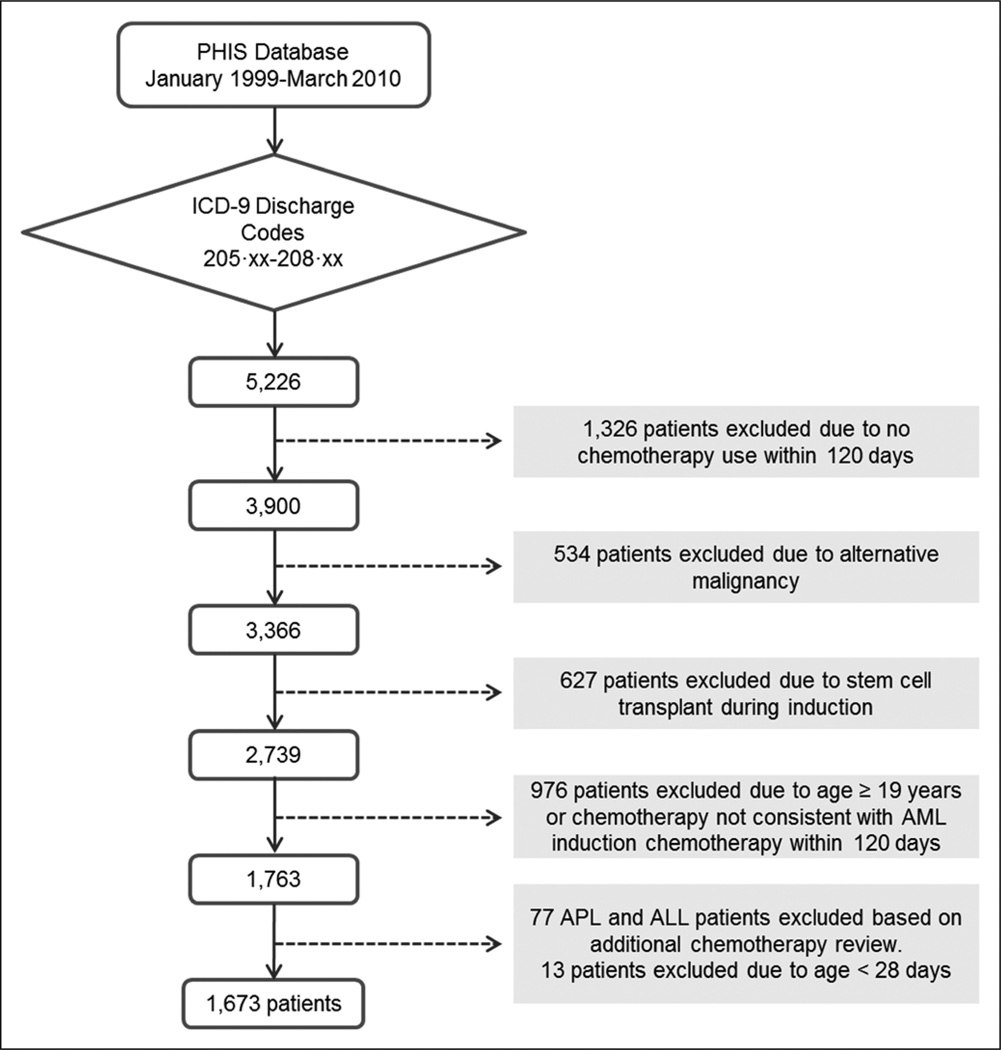
Patients who are newly diagnosed with acute myeloid leukemia and who are 28 days through 18 years old (n = 1,673) hospitalized any time from initial diagnosis through 9 months following diagnosis or until stem cell transplant. A reference cohort of all nononcology pediatric admissions using the same intensive care resources in the same time period (n = 242,192 admissions) was also studied.
None.
One-third of pediatric patients with acute myeloid leukemia (553 of 1,673) required intensive care during a hospitalization within 9 months of diagnosis. Among intensive care admissions, mortality was higher in the acute myeloid leukemia cohort compared with the nononcology cohort (18.6% vs 6.5%; odds ratio, 3.23; 95% CI, 2.64-3.94). However, when sepsis was present, mortality was not significantly different between cohorts (21.9% vs 19.5%; odds ratio, 1.17; 95% CI, 0.89-1.53). Mortality was consistently higher for each type of organ failure in the acute myeloid leukemia cohort versus the nononcology cohort; however, mortality did not exceed 40% unless there were four or more organ failures in the admission. Mortality for admissions requiring intensive care decreased over time for both cohorts (23.7% in 1999-2003 vs 16.4% in 2004-2010 in the acute myeloid leukemia cohort, p = 0.0367; and 7.5% in 1999-2003 vs 6.5% in 2004-2010 in the nononcology cohort, p < 0.0001).
Pediatric patients with acute myeloid leukemia frequently required intensive care resources, with mortality rates substantially lower than previously reported. Mortality also decreased over the time studied. Pediatric acute myeloid leukemia patients with sepsis who required intensive care had a mortality comparable to children without oncologic diagnoses; however, overall mortality and mortality for each category of organ failure studied was higher for the acute myeloid leukemia cohort compared with the nononcology cohort.
儿童急性髓系白血病患者有发生脓毒症和器官衰竭的风险。在大型儿科急性髓系白血病患者人群中,尚未研究强化治疗支持的相关预后。我们的目的是确定需要重症监护的儿科急性髓系白血病患者的院内死亡率。
1999 年至 2010 年间住院的儿童进行的回顾性队列研究。通过使用特定的程序和资源来定义重症监护的使用。主要终点是院内死亡率。
向儿科健康信息系统数据库提供数据的 43 家儿童医院。
新诊断为急性髓系白血病且年龄在 28 天至 18 岁之间的患者(n=1673),自初次诊断起至诊断后 9 个月或直至进行干细胞移植期间任何时间住院。同时研究了在同一时期内使用相同重症监护资源的所有非肿瘤儿科住院患者(n=242192 例)的参考队列。
无。
三分之一的儿科急性髓系白血病患者(1673 例中的 553 例)在诊断后 9 个月内的住院期间需要重症监护。在重症监护病房中,急性髓系白血病组的死亡率明显高于非肿瘤组(18.6% vs 6.5%;比值比,3.23;95%置信区间,2.64-3.94)。然而,当发生脓毒症时,两组之间的死亡率没有显著差异(21.9% vs 19.5%;比值比,1.17;95%置信区间,0.89-1.53)。在急性髓系白血病组中,每种类型的器官衰竭的死亡率均明显高于非肿瘤组;然而,除非在入院时出现四种或更多种器官衰竭,否则死亡率不会超过 40%。在需要重症监护的住院患者中,死亡率在急性髓系白血病组和非肿瘤组中均随时间逐渐降低(急性髓系白血病组 1999-2003 年为 23.7%,2004-2010 年为 16.4%,p=0.0367;非肿瘤组 1999-2003 年为 7.5%,2004-2010 年为 6.5%,p<0.0001)。
儿科急性髓系白血病患者经常需要重症监护资源,死亡率远低于之前报道的水平。死亡率也随研究时间的推移而降低。需要重症监护的伴有脓毒症的急性髓系白血病患儿的死亡率与无肿瘤诊断的患儿相似;然而,与非肿瘤组相比,急性髓系白血病组的总体死亡率和每个研究器官衰竭类别的死亡率更高。